
 |
Why does a patient with epilepsy, seizure free for 12 years off antiepileptic drugs (AEDs), suddenly develop breakthrough seizures? The case of S.J., a patient with recurrent medically intractable seizures, demonstrates the merit of pursuing evaluation for possible comorbid sleep disorders.
BACKGROUND
Breakthrough seizures in patients with known epilepsy are not uncommon. Typical etiologies for breakthrough seizures include AED noncompliance, initiation of a new medication that interferes with AEDs or is proconvulsant, concomitant infection, increased stress level, or a change in sleep pattern (eg, sleep deprivation). If no clear provoking factors are present and if there is a pattern of recurrence, AEDs may need to be adjusted. The longer a patient remains seizure-free, the less likely they are to have breakthrough seizures.1

Have a case report you would like to share? E-mail us at |
PATIENT CASE
S.J. is a 28-year-old, right-handed man with a history of autism, mental retardation, and meningitis at birth. Soon after birth, he developed two seizure types. The first type consisted of brief staring spells associated with a behavioral arrest. The second type consisted of a sudden onset of whole body convulsions with a duration of as long as 2 minutes. He was diagnosed with symptomatic generalized epilepsy and then treated with AEDs. Seizures stopped spontaneously at 16 years of age. He continued to take AEDs for an additional 2 years, and then they were discontinued. He remained seizure-free off of AEDs until 28 years of age when seizures recurred.
His current seizures began 4 months ago and occur during sleep after loud snores and periods of hesitation in breathing pattern. Seizure semiology is described as a sudden onset of whole body stiffening associated with jerking for a duration of up to 2 minutes. He then has postictal tremor and gait instability. An outpatient routine awake electroencephalogram (EEG) demonstrated interictal paroxysmal generalized spikes and spike wave discharges without clinical manifestations. He was diagnosed with recurrent epileptic seizures and started on phenytoin. Multiple nightly seizures continued despite the addition of phenobarbital. Because seizures were preceded by snoring, S.J. was referred for a sleep evaluation.
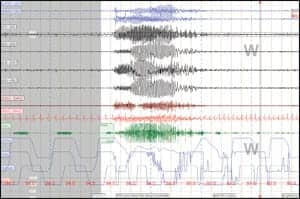 |
| Figure 1. Initial PSG. Seizure one, 30-second epoch. Snore-associated generalized seizure on EEG with clinical generalized tonic-clonic activity. |
According to his grandmother, in the last year S.J. had gained 50 pounds and developed new onset leg swelling. During sleep, he had very loud snoring, witnessed apneic events, and frequent nocturia. He complained of occasional night sweats and awoke several times during the night with shortness of breath. Nocturnal seizures and snoring were worse when supine. He averaged 9.5 hours of sleep with fairly consistent bedtimes and arising times. Upon awakening, he did not feel refreshed and complained of dry mouth and daytime sleepiness. His grandmother often caught S.J. asleep due to inadvertent naps. His Epworth Sleepiness Score (ESS) was 16/24 indicating excessive daytime sleepiness. He denied daytime seizures.
On general exam, S.J. was obese and normotensive, and had dysmorphic facial features. He had a large tongue and was unable to fully close his mouth. He had excessive drooling and carried a towel with him to keep the front of his shirt dry. His posterior oropharynx was crowded, and he had an increased neck size. His bilateral distal lower extremities had mild nonpitting edema. Neurologically, he was friendly, cooperative, and able to follow simple commands. He demonstrated decreased fund of knowledge, dysarthric speech, and imbalance during nonstressed gait and turns.
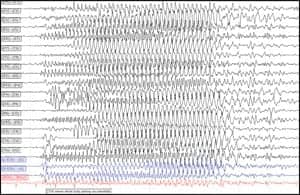 |
| Figure 2. Initial PSG. Seizure one, 10-second epoch, extended EEG anterior-posterior bipolar montage. Snoreassociated generalized seizure with clinical generalized tonic-clonic activity. |
DIAGNOSIS
Cardiac evaluation demonstrated normal findings on electrocardiogram, transthoracic echocardiogram, and 24-hour pulse oximetry tests. Nocturnal polysomnogram (PSG) with extended EEG demonstrated very loud snoring and significant obstructive sleep apnea (OSA). His respiratory events were associated with arousals and oxygen desaturation as low as 86%, worse in the supine position. He had 24 snore events associated with immediate onset of generalized tonic-clonic convulsions lasting 9 to 20 seconds. All of the convulsions occurred during non-REM sleep. Clinical seizure activity correlated with generalized spikes on EEG (see Figures 1 and 2). There were no non-respiratory-associated epileptiform discharges, or electrographic or clinical seizures. These generalized seizures were felt to be provoked by the respiratory disturbances.
A repeat PSG with continuous positive airway pressure (CPAP) titration was ordered for treatment of his obstructive sleep apnea. The CPAP titration PSG demonstrated improvement of his sleep-disordered breathing on 10 cm of water with a full face mask. There were only six snore-related events associated with electrographic rhythmic generalized spikes on EEG. All six electrographic seizures were less than 4 seconds and were not associated with clinical manifestations (see Figures 3 and 4, page 24). There were no other epileptiform discharges or electrographic seizures during the CPAP titration PSG. He tolerated CPAP well and felt better than usual upon awakening.
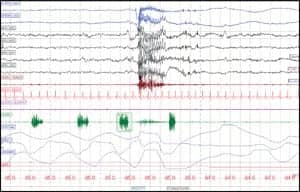 |
| Figure 3. CPAP titration PSG. Seizure one, 30-second epoch. Snore-associated rhythmic electrographic epileptiform discharges without clinical manifestations. |
TREATMENT
S.J. was prescribed CPAP 10 cm of water with a full face mask. His AEDs were maintained. During his 1-month follow-up evaluation, his grandmother reported S.J. had adjusted well to CPAP. He felt more rested in the mornings and had some decreased daytime sleepiness. His snoring and apneic events were controlled, and he was seizure-free. During each subsequent follow-up visit, including his most recent 8-month visit, his grandmother reported continued improvement with resolution of snoring, apneic events, peripheral edema, and daytime sleepiness with a score (<10) on the ESS. Additionally, he remained seizure-free.
DISCUSSION
When patients with epilepsy develop breakthrough seizures, it is important to evaluate for common provoking factors. This includes disrupted sleep. Multiple awakenings during sleep disrupt sleep architecture and can lead to sleep deprivation and daytime sleepiness. Sleep deprivation may lower the seizure threshold by increasing cortical excitability.2 There are many causes of sleep deprivation including inadequate sleep hygiene, insufficient sleep syndrome, nocturnal epileptiform discharges or seizures, and other primary sleep disorders such as OSA, restless legs syndrome, insomnia, and parasomnias.3
Factors that contribute to disrupted sleep can lead to daytime sleepiness. Increased daytime sleepiness may lead to long naps, and thus may contribute to insomnia and circadian rhythm dysfunction. Excessive daytime sleepiness is common in patients with epilepsy.3-9 Epilepsy and its treatment can influence sleep organization.5,10,11 Seizures during the day and during sleep can disrupt sleep architecture. One study of patients with seizures during sleep demonstrated subsequent reduced REM sleep, increased NREM stage 1 sleep, and decreased daytime alertness. Seizures during the day also reduced REM sleep the following night.10,12
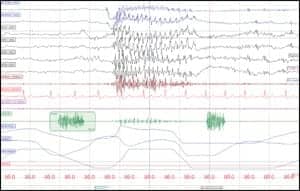 |
| Figure 4. CPAP titration PSG. Seizure one, 10-second epoch. Snore-associated rhythmic electrographic epileptiform discharges without clinical manifestations. |
Additionally, AEDs may affect sleep architecture and induce somnolence. Gabapentin increases slow wave sleep in normal adults.13 Lamotrigine increases REM sleep, and reduces stage shifts and arousals in patients with focal epilepsy.14,15 Barbiturates and benzodiazepines decrease sleep latency and arousals; however, they decrease REM sleep in patients with epilepsy.13 Most AEDs may increase daytime somnolence.4,12,15 Lamotrigine, zonisamide, phenytoin, ethosuximide, and felbatol have been associated with insomnia.4,12
In addition to direct effects on sleep, some AEDs may have secondary effects on sleep. Many AEDs are associated with weight gain.4,6,16 Obesity is a known risk factor for OSA. Additionally, carbamazepine has been associated with exacerbation of periodic limb movements during sleep.4,12 Several antiepileptic drugs, including gabapentin, are commonly used off-label for treatment of restless legs syndrome and/or periodic limb movement disorder.4,17
Screening for comorbid sleep disorder symptoms can be assessed quickly during an outpatient visit. Focused sleep history should inquire about the presence of daytime sleepiness, bedtimes and arising times, difficulty initiating and maintaining sleep, snoring, observed apneas during sleep, unrefreshed awakenings, restless legs symptoms, and nocturnal behaviors or seizures. The ESS is an eight-question tool used to measure the propensity of falling asleep in several daytime settings. ESS scores range from 0 to 24 points with scores of greater than 10 associated with increased sleepiness.18 In a population of patients with epilepsy, abnormal ESS (>10) correlated with loud habitual snoring, witnessed apneas, and recurrence of seizures within the last 12 months.7 If sleep history is positive, further investigation (eg, laboratory studies, PSG) and treatment may be warranted.
There are several studies noting the common occurrence of OSA in patients with epilepsy.3,6-8,16,19 Treatment of OSA in these patients resulted in improved seizure control8,20-22 and quality of life.9,16 Our patient developed recurrent seizures after many years of seizure freedom. He also had daytime sleepiness, significant weight gain, and signs and symptoms of OSA. Polysomnographic evaluation diagnosed significant OSA and respiratory event-associated generalized tonic-clonic seizures. Nocturnal seizures and OSA can disrupt sleep architecture and lead to sleep deprivation and daytime sleepiness. CPAP titration PSG demonstrated a 75% reduction in frequency of respiratory event-associated electrographic epileptiform activity and total resolution of clinical seizures. Continued CPAP therapy controlled OSA symptoms and clinical seizures.
This case study demonstrates the importance of evaluating for comorbid sleep disorders in patients with epilepsy who develop breakthrough seizures. Sleep evaluation may lead to the diagnosis of a comorbid sleep disorder, thus revealing a contributing factor for the development of breakthrough seizures. Treatment of comorbid sleep disorders may improve seizure control, sleep, and quality of life.
Jennifer L. DeWolfe, DO, is an assistant professor of neurology at the University of Alabama at Birmingham. She is the director of UAB Neurology Sleep Services and of the Birmingham Veterans Affairs Sleep Center. She is board certified by the American Board of Psychiatry and Neurology and specializes in epilepsy and sleep medicine. Contact her at [email protected].
REFERENCES
- Chadwick D, Taylor J, Johnson T. Outcomes after seizure recurrence in people with well-controlled epilepsy and the factors that influence it. The MRC Antiepileptic Drug Withdrawal Group. Epilepsia. 1996;37(11):1043-50.
- Badawy RA, Curatolo JM, Newton M, Berkovic SF, Macdonell RA. Sleep deprivation increases cortical excitability in epilepsy: syndrome-specific effects. Neurology. 2006;67(6):1018-22.
- Bazil CW. Sleep, sleep apnea, and epilepsy. Curr Treat Options Neurol. 2004;6(4):339-345.
- Bazil C. AEDs, sleep, and epilepsy. October 1, 2007. http://www.epilepsy.com/articles/ar_1191272878:[. Accessed August 15, 2008.
- Dinner DS. Effect of sleep on epilepsy. J Clin Neurophysiol. 2002;19(6):504-13.
- Malow BA, Bowes RJ, Lin X. Predictors of sleepiness in epilepsy patients. Sleep. 1997;20(12):1105-10.
- Manni R, Politini L, Sartori I, Ratti MT, Galimberti CA, Tartara A. Daytime sleepiness in epilepsy patients: evaluation by means of the Epworth sleepiness scale. J Neurol. 2000;247(9):716-7.
- Vaughn BV, Miller MT, D’Cruz OF, Messenheimer J. Prevalence of sleep complaints in patients with epilepsy: application of the Epworth sleepiness scale. J Sleep Res. 1996;25:453.
- Piperidou C, Karlovasitou A, Triantafyllou N, et al. Influence of sleep disturbance on quality of life of patients with epilepsy. Seizure. 2008;17(7):588-94.
- Bazil CW, Castro LH, Walczak TS. Reduction of rapid eye movement sleep by diurnal and nocturnal seizures in temporal lobe epilepsy. Arch Neurol. 2000;57(3):363-8.
- Kotagal P, Yardi N. The relationship between sleep and epilepsy. Semin Pediatr Neurol. 2008;15(2):42-9.
- Adverse reactions to antiepileptic drugs: a multicenter survey of clinical practice. Collaborative Group for Epidemiology of Epilepsy. Epilepsia. 1986;27(4):323-30.
- Foldvary-Schaefer N, De Leon Sanchez I, Karafa M, Mascha E, Dinner D, Morris HH. Gabapentin increases slow-wave sleep in normal adults. Epilepsia. 2002;43(12):1493-7.
- Foldvary N, Perry M, Lee J, Dinner D, Morris HH. The effects of lamotrigine on sleep in patients with epilepsy. Epilepsia. 2001;42(12):1569-73.
- Placidi F, Marciani MG, Diomedi M, et al. Effects of lamotrigine on nocturnal sleep, daytime somnolence and cognitive functions in focal epilepsy. Acta Neurol Scand. 2000;102(2):81-6.
- Bazil CW. Sleep and epilepsy. Curr Opin Neurol. 2000;13(2):171-5.
- Satija P, Ondo WG. Restless legs syndrome: pathophysiology, diagnosis and treatment. CNS Drugs. 2008;22(6):497-518.
- Johns MW. A new method for measuring daytime sleepiness: the Epworth sleepiness scale. Sleep. 1991;14(6):540-5.
- Chihorek AM, Abou-Khalil B, Malow BA. Obstructive sleep apnea is associated with seizure occurrence in older adults with epilepsy. Neurology. 2007;69(19):1823-7.
- Devinsky O, Ehrenberg B, Barthlen GM, Abramson HS, Luciano D. Epilepsy and sleep apnea syndrome. Neurology. 1994;44(11):2060-4.
- Hollinger P, Khatami R, Gugger M, Hess CW, Bassetti CL. Epilepsy and obstructive sleep apnea. Eur Neurol. 2006;55(2):74-9.
- Wyler AR, Weymuller EA Jr. Epilepsy complicated by sleep apnea. Ann Neurol. 1981;9(4):403-4.





{kind=link}