
The purpose of this article is to identify performance variables of the five APAP devices.
After 25 years since the first description of CPAP, titration for treatment of obstructive sleep apnea remains surprisingly not evidence based. Adding to this observation, Rodenstein comments in his 2008 editorial1 that manual titration is still an art and auto-adjusting positive airway pressure (APAP) seems to fail so frequently that it may be unreliable as a means to improve compliance or serve as a diagnostic device. These bold statements are justified by his review of the evidence and the wide variability of performance of APAP devices that impact consistent therapy. These comments should challenge clinicians to understand the issues surrounding APAP therapy and promote more “why” and “how” questions related to product capabilities and the science behind the performance and capabilities of devices used to treat obstructive sleep apnea.
One of the first APAP devices was introduced in France in 1962.2 The intent of the device was to reduce mean airway pressure to make CPAP therapy more comfortable and improve patient compliance. The device was designed and developed based on an estimate of appropriate pressure, estimates of flow changes, possible breathing disorder, and a little SWAG (scientific wild ass guess). There was no way for the early developers to have an established base for the technology as it was a new approach to a sleep-disordered breathing event. The product was tested with positive results related to improved patient compliance. Was this exhaustive or complete evidence-based research? Further research discovered that the flow-based breathing signal could identify breathing patterns that could assist in the understanding of disorganized breathing patterns and add another feature for diagnostic as well as therapeutic value to APAP. Again, there were studies that confirmed the capabilities of the device to provide a diagnostic option. Was this exhaustive or complete evidence-based research?
Series et al discussed in his 2008 article3 that there are significant differences in performance between APAP devices for both 1-night and 1-week titration and warned that important discrepancies in the effective pressure can alter CPAP compliance and efficiency. In Lofaso’s bench evaluation of five APAP devices,4 he concluded that physicians need details on the algorithm used in each APAP device and that manufacturers should provide that data. There continues to be a lack of data on both the mechanical and clinical performance of individual APAP devices, and most of the device algorithms were based on a flurry of research in 19985-7 that was used by many of the manufacturers to base their auto-adjusting algorithm with little change or adjustment since that time.
Many Questions, Few Answers
Today, in the US market, there are five commercially available APAP devices that provide clinicians with the means to diagnose and treat sleep-disordered breathing.
- Do clinicians know of the performance differences?
- Is there current, objective research identifying the capabilities and limitations of each device?
- Does the clinician select the appropriate device knowing its capabilities for a specific patient and monitor the patient for the desired outcomes?
- Is anyone asking questions about these devices related to their capabilities and the evidence-based research that has documented the specific performance of the devices before they are purchased and used on patients?
The purpose of this article is to identify performance variables of the five APAP devices and challenge the reader to ponder these questions.
APAP devices are considered a commodity by many clinicians. The general consensus is that all APAPs are capable of providing positive results and the only consideration for determining which device to choose is features and price. Our research has determined that all APAPs are different, based on the algorithm that controls the device’s response to a breathing signal.8 The devices are not commodities and are significantly different in pressure response. How would the clinician know of these performance variables? Product literature does not identify how a device will respond to a breathing signal. There are no standards established for the appropriate pressure response to a specific breathing pattern as there do not seem to be research sites or standards agencies that are looking at this issue. If there are no standards and no research, how does one know if a product is providing the results expected from these devices? Monitoring positive outcomes is the standard response from many clinicians, yet if all devices perform differently and clinicians indicate that the device they have selected provides positive outcomes, is it possible that each clinician has purchased the correct device for their patient population? Are patient populations that well segmented to allow for this phenomenon, and have all the different APAP devices been put on the proper patients for these positive results? Unlikely!
The sleep apnea therapy market is moving too quickly for research to keep up with market changes, economics, and product development. New products are entering the market at a rapid pace and being positioned as the latest and greatest products for the sleep-deprived patient. New payor regulations are challenging the provider to identify new methods of providing products and services with the goal of reduced costs. Without evidence of positive results from the therapy, overall cost may be higher with the goal of effectively treating sleep apnea falling short and the prevention of complications not achieved.
Comparative Bench Testing of 5 APAP Devices
Bench testing was conducted a few years ago by our group on the four then commercially available APAP devices.8 Recently, a new APAP was introduced to the market and our group wanted to determine this new device’s capability and retest the other devices to see if there were any algorithm changes to the existing units. The test process was similar to the 2006 bench testing method.
Method
Prior to this test, four sleep-disordered breathing patterns were taken from nasal pressure data collected on patients who had undergone a polysomnography study and scored by a professional RPSGT. Normal, apnea, flow-limitation, and hypopnea patterns were digitized for use by a mechanical test lung (Series 1101 Breathing Simulator, Hans Rudolph Inc). The amount of data converted for each pattern varied, with the flow-limitation pattern totaling approximately 8 minutes in length and the hypopnea pattern totaling approximately 12.5 minutes in length. Both the normal and apnea breathing patterns were approximately 10 minutes in length. Each file and script were set to loop back to start at the conclusion of the recorded sample to allow for a 30-minute test run. While the disordered breathing patterns are scored as apnea, flow limitation, and hypopnea, there may be incidences of one type present in another signal, such as flow-limited breaths in the hypopnea signal. Shown at left are 50-second samples of each type of sleep-disordered breathing pattern recorded and applied to each APAP device.
Results
All APAP units were able to complete all tests as outlined in the protocol with no complications.
Common in the Respironics APAP models is a “hunt and peck” search pattern, as part of the device’s algorithm is to find optimum therapy pressures in the face of airway resistance. The unit will increase pressure by 1.5 cm H2O over the course of 3 minutes and monitor the flow to see if there is an improvement. If there is none, the unit returns to the original pressure within 1 minute. If an improvement is recorded during the 1.5 cm H2O pressure increase phase, the device will lower the pressure by only 0.5 cm H2O. As there is no physiological component in this bench test, the unit consistently returned to the original pressure setting during periods of normal breathing. These are seen in the resulting device pressure profiles as triangular pressure increases/decreases.
 |
| Figure 1 |
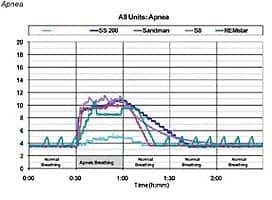
Apnea. All devices exhibited pressure response to the change from normal to apneic breathing (Figure 1). The SleepStyle 220 (Fisher & Paykel), Sandman (Covidien), and S8 units (ResMed) rapidly responded to the apnea pattern, achieving the 10 cm H2O default apnea cap programmed for these units within 5 minutes of the apnea pattern starting; the REMstar unit achieved 10 cm H2O within 10 minutes. The SleepStyle 200, Sandman, and S8 units all increased pressure above 10 cm H2O, suggesting a pressure response to other nonapneic events present in the signal. The intelliPAP (DeVilbiss) unit responded less quickly, achieving a maximum therapy pressure of 5.5 cm H2O by the end of the 30-minute apnea session. The REMstar (Respironics) unit showed an instantaneous drop of 2 cm H2O to 8.5 cm H2O about 12 minutes into the apnea pattern, where it remained for the next 15 minutes. This is a programmed response by the device as its algorithm has recognized that there is no response from the “patient” to the sudden increases in pressure. The drop in pressure is to ensure the patient is not receiving too high a pressure in the event that the apnea is central in nature, possibly resulting in a Hering-Breuer reflex. The return to the initial pressure once normal breathing resumed varied for each unit with quicker reductions in pressures occurring on the Sandman and REMstar units compared to the more gradual pressure decreases on the intelliPAP, S8, and SleepStyle 200 units.
 |
| Figure 2 |
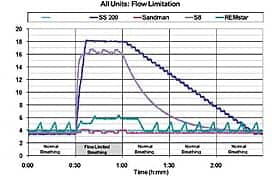
Flow Limitation. Both the SleepStyle 200 and S8 units showed a rapid response to the flow-limitation breathing pattern (Figure 2). The initial peak therapy pressures were achieved within 5 minutes of the change from normal breathing to flow-limited breathing. The intelliPAP, Sandman, and REMstar unit responded much differently, showing little change in pressures over the 30 minutes, with the IPAP AA unit not changing delivered pressure at all. Based on the REMstar algorithm’s search feature, the unit appeared to note an improved flow signal, as there were two instances of the device increasing pressure by 1.5 cm H2O and then dropping pressure by 0.5 cm H2O shortly thereafter during the flow-limited segment. Again, the return to the initial therapy pressure once normal breathing resumed varied for the two units that showed response to the flow-limitation pattern, though both were more gradual in nature.
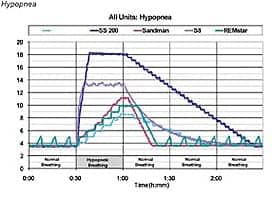
Hypopnea. All devices exhibited a response to the change from normal to hypopneic breathing (Figure 3). Again, the SleepStyle 200 and S8 units showed a rapid response, quickly reaching initial peak pressures within 5 to 7 minutes. The intelliPAP, Sandman, and REMstar unit exhibited similar, steady rises in therapy pressure throughout the 30-minute session with maximum pressures between 10 and 12 cm H2O. As with the other two disordered patterns tested, the return to the initial therapy pressure once normal breathing resumed varied for each unit, with the IntelliPAP, SleepStyle 200, and S8 units employing a more gradual decrease in therapy pressure compared to the Sandman and REMstar unit.
 |
| Figure 3 |
Except for the individual manufacturer, no one knows how these algorithms were determined, tested, and validated for effectiveness. The variability of product performance and the unknown aspect of how the algorithms determine response suggest that the manufacturers should publicly specify the characteristics of the abnormal flow pattern detection and the algorithms used by their devices to respond to the abnormal flow.4 The sophistication of the algorithm for each device may include individual responses to a combination of signals and snoring to determine how the device will respond. This study is limited in that the units tested were provided only one particular sample of each type of disordered breathing pattern for apnea, hypopnea, and flow limitation, and none of these included a snore signal. As all units feature snoring detection capabilities, the lack of a snoring component may have contributed to the minimal response on the part of the intelliPAP, REMstar, and Sandman units in the flow-limitation pattern.
Manufacturer Responses
All five of the manufacturers of auto-adjusting devices included in our comparison were given the opportunity to respond to three principal questions regarding the companies’ approaches to algorithm design. All manufacturers, with the exception of Covidien, responded to the questions. The following is a summary of the responses:
Question 1: Please generally summarize the approach used in your auto-adjust CPAP machine’s algorithm to detect sleep-disordered breathing events?
a. All four respondents indicate that the algorithm uses a proactive approach by analyzing the airway’s potential to collapse, prior to an event being detected. This is primarily based on the detection of flow limitation or snoring by utilizing “flow based analysis.”
b. All four respondents indicate that the algorithm is able to identify flow limitation, snoring, hypopnea, and apnea.
c. Only one respondent (Respironics) describes a goal of always delivering the lowest CPAP pressure possible.
d. All four respondents indicate the algorithm is capable of distinguishing central versus obstructive events in order to avoid pressure increase for nonresponding events.
Question 2: How does your product respond once a sleep-disordered breathing event is detected?
a. All four respondents indicate that if an event such as apnea or hypopnea is detected, it is assumed that the device will have already detected the potential for the events through flow-based analysis and a pressure above the minimum will already be in effect. The device will then respond with mild increases in pressure until the events cease.
b. One of the four respondents describes a sliding 5-minute analysis window.
c. One of the four respondents (Fisher & Paykel) indicates the algorithm’s ability to determine the severity level of a particular event, and the response of the device will vary depending on the severity of the event.
d. Another (ResMed) describes a five-breath moving average analysis window.
Question 3: What was the basis or reference for incorporating the above-described approach to detecting and responding to sleep-disordered breathing events?
a. One of the four respondents (Respironics) indicates that the algorithm is largely based on clinical understanding and practices used in titrating CPAP pressures during a PSG titration process.
b. All four respondents indicate that research published throughout the 1990s is the principal reference used in developing the algorithm.
Unanswered Questions
All of the manufacturers’ responses were largely similar relating to approaches and strategies incorporated into their respective algorithms. If the algorithms are similar, why do the devices respond in such dramatically different ways to a fixed stimulus of sleep-disordered breathing events?
The manufacturer’s description of algorithms indicates that the intended use of the device is within a long-term therapeutic application. However, these devices are commonly used by sleep labs as “bed extenders” in situations where incomplete titration data was experienced during PSG testing. An average or mean pressure reported by the device after 2 or 3 weeks of home use is then used with a fixed pressure machine for long-term therapy. Should the devices be used in this manner considering the long-term therapy-based approaches used within the algorithms?
Why did the devices’ responses change over the 3-year interval of this testing. Were the changes based on new research? Should patients using the older algorithm upgrade?
Conclusion
Since their introduction more than 15 years ago, APAP units have become an increasingly popular option for use in sleep therapy. Used as both a means of improving patient compliance with therapy due to an overall lower mean airway pressure or an application as a bed extender for sleep labs to identify fixed therapeutic CPAP pressures, these units are seeing more utilization. Testing has revealed that the performance characteristics of the units are significantly different in response to various sleep-disordered breathing patterns. There is little comparative research on the use and benefits of the individual devices so the scientific evidence for the devices is lacking. How then does a clinician determine which brand to select for their patient populations? What questions does the clinician ask the manufacturer related to the product’s capabilities and the objective data to support marketing claims? Especially in light of the recent growth in unattended in-home sleep testing programs that utilize APAP units exclusively, these questions should certainly be considered and addressed. Clinicians working in the OSA arena need to meet patients’ expectation that they are being treated effectively with the best diagnostic process and effective therapy.
Robert McCoy, RRT, is managing director, and Ryan Diesem, BS, is the research associate, Valley Inspired Products Inc, Apple Valley, Minn. Todd Eiken, RPSGT, is technical director, Mays and Associates Inc, St Paul, Minn.
REFERENCES
- Rodenstein D. Determination of therapeutic continuous positive airway pressure for obstructive sleep apnea using automatic titration: promises not fulfilled. Chest. 2008;133:595-7.
- Meurice JC, Marc I, Series F. Efficacy of auto CPAP in the treatment of obstructive sleep apnea/hypopnea syndrome. Am J Respir Crit Care Med. 1996;153:794-8.
- Series F, Plante J, Lacasse Y. Reliability of home CPAP titration with different automatic CPAP devices. Respir Res. 2008;9:56.
- Lofaso F, Desmarais G, Leroux K, et al. Bench evaluation of flow limitation detection by automated continuous positive airway pressure devices. Chest. 2006;130:343-9.
- Teschler H, Berthon-Jones M. Intelligent CPAP systems: clinical experience. Thorax. 1998;53(suppl):S49-54.
- Ayappa I, Norman RG, Hosselet JJ, Gruenke RA, Walsleben JA, Rapoport DM. Relative occurrence of flow limitation and snoring during continuous positive airway pressure titration. Chest. 1998;114:685-90.
- Berkani M, Lofaso F, Chouald C, et al. CPAP titration by an auto CPAP device based on snoring detection: a clinical trial and economic considerations. Eur Respir J. 1998;12:759-63.
- McCoy R, Eiken T. Created unequal. Sleep Review. May/June 2006. Accessed June 3, 2009.
APAP Bench Test: Vendors Respond
Sleep Review: In a couple of brief paragraphs, please generally summarize the approach used in your auto-adjust CPAP machine’s algorithm to detect sleep-disordered breathing events?
Fisher & Paykel: The Fisher & Paykel Healthcare SleepStyle™ 200 Auto Series device uses a flow-based auto-adjusting algorithm, designed to detect and respond to flow limitation, hypopnea, and apnea.
The research clearly shows that flow limitation is a strong precursor to upper airway collapse. Therefore, detection and elimination of flow limitation prevent more severe indices of sleep-disordered breathing (SDB) from occurring, such as apnea or hypopnea. Complex statistical analysis of each breath allows us to accurately detect flow-limited breathing.
An additional algorithm called SensAwake™ has also been incorporated into this device to enhance comfort during wakefulness. Patients are often intolerant of the pressure while they are awake, and it is during this time that comfort is critical for long-term use. SensAwake is a sophisticated pressure relief technology that detects the transition from sleep to awake and promptly reduces the pressure in order to aid the transition back to sleep. SensAwake, combined with Ambient Tracking™ Plus humidification technology, works to enhance the comfort and performance of the auto-adjusting algorithm for improved therapy acceptance and clinical outcomes.
DeVilbiss: The DeVilbiss IntelliPAP® AutoAdjust® is a flow-based autotitrator that senses and categorizes events as either responding and nonresponding events (ie, potential central events). The AutoAdjust will increase pressure to detected responding events and will maintain pressure to nonresponding events, because a pressure response may complicate the event. Once breathing stabilizes, the AutoAdjust will reduce the pressure gradually to avoid arousals.
The responding events are snoring, obstructive apneas, and hypopneas. The algorithm analyzes flow patterns the same way a sleep technician would visually identify respiratory events during a sleep study. Snoring is defined as an interruption of the flow signal on inspiratory waveform. Obstructive apneas are defined by a major decrease in the amplitude of the total respiratory waveform, and hypopneas are defined by a partial reduction of the respiratory waveform. A unique feature of the DeVilbiss AutoAdjust algorithm is the ability to change the sensitivity of the algorithm by changing definitions of respiratory events, almost creating a customized algorithm.
ResMed: The treatment pressure required by a patient may vary through the night—and from night to night—due to changes in sleep state, body position, and airway resistance. Pressure needs for maintaining an open upper airway in a sleep apnea patient can also be influenced by long-term variance due to weight gain or loss and use of alcohol or pharmaceuticals.
ResMed’s AutoSet™ algorithm monitors the patient on a breath-by-breath basis to maintain upper airway patency for any given breath. The AutoSet algorithm adjusts treatment pressure as a function of three parameters: inspiratory flow limitation, snore, and apnea. By analyzing inspiratory flow limitation in minute detail during each respiratory cycle, the AutoSet algorithm is able to detect and distinguish obstructive hypopnea from central hypopnea: the AutoSet algorithm is able to detect and treat obstructive hypopnea (with flow limitation) and detect and record central hypopnea (without flow limitation) events. These three lines of defense allow the AutoSet algorithm to treat the patient effectively, as the patient needs it, throughout the night.
Philips Respironics: The main goal of the REMstar Auto algorithm is to normalize sleep by delivering the lowest CPAP pressure. What makes the REMstar Auto algorithm unique is its sophisticated three-layered algorithm. Unlike other auto-titrating devices in the market, the REMstar Auto can manage a respiratory event in the early stages rather than waiting for it to occur.
The primary function of the algorithm is to conduct a proactive analysis of the patient’s upper airway and its potential to collapse. It makes subtle, programmed CPAP pressure adjustments in response to detected changes in flow.
The second layer consists of programmed responses to apneas, hypopneas, flow limitations, and vibratory snores.
In the third layer, the algorithm operates in a variety of exception conditions. For example, the algorithm ceases to increase pressure for patients who may experience sleep-disordered breathing events that are not responsive to pressure increases (such as central apneas). The algorithm decreases CPAP pressure when the patient is experiencing a large mask leak. The result is clinically proven, effective therapy at minimal CPAP pressure.
Sleep Review: How does your product respond once a sleep-disordered breathing event is detected?
Fisher & Paykel: Once a sleep-disordered breathing event is detected, the pressure increase will vary according to the severity of the event and the current pressure. For example, the device will respond more aggressively to an apnea than to a hypopnea or flow-limitation event.
An important factor that will impact the response of the auto algorithm is the apnea-cap setting. The apnea cap is designed to prevent unnecessary pressure increases due to central events. The apnea cap is a changeable parameter that by default is set to 10 cm H2O . Below the apnea-cap pressure, the device will respond to all forms of sleep-disordered breathing. At or above this pressure, the device will only respond to SDB events that are clearly obstructive in nature, ie, events associated with flow limitation.
DeVilbiss: As the cycle of sleep apnea begins, a precursor to obstructive apneas and hypopneas is snoring. The DeVilbiss AutoAdjust algorithm senses snoring and begins to increase the pressure prior to obstructive apneas and hypopneas in an attempt to prevent these events from occurring. The patient may still have apneas and hypopneas, especially during REM or while in a supine position during the night. There is a need to respond to apneas and hypopneas as they occur during a patient’s sleep cycle to keep the airway patent. Dynamic changes in pressure are able to keep the airway open as the patient needs change.
ResMed: The AutoSet algorithm is truly a predictive approach allowing proactive treatment of sleep apnea rather than simply reacting with a pressure change after an event has occurred; this is achieved by detailed analysis of the inspiratory flow versus time curve. Flow limitation analysis in the AutoSet algorithm is a complex blend of clinical sleep science and engineering; it provides very small adjustments in pressure, sometimes as little as 0.2 cm H2O at a time to ensure that the patient is not aroused from sleep (as measured by EEG) with such pressure changes. This approach allows AutoSet to preemptively treat many obstructive sleep apnea events before they even occur. When an event does occur that is not possible to prevent by the flow limitation approach, AutoSet will respond reactively as well. ResMed’s AutoSet algorithm assesses the severity of the event using a blend of the inputs such as duration of the event severity and frequency of the event over time. The AutoSet algorithm then determines the optimal pressure change solution to treat the event and prevent future events and applies it comfortably with minimal disturbance to the patient’s sleep.
AutoSet responds to events based on a five-breath moving average of the inspiratory flow-time curve in order to prevent the device from responding to sporadic breathing events, such as sighs or coughs. Inspiratory flow limitation, or partial airway closure, usually precedes snoring and obstructive hypopnea and apnea events; it is also most often associated with obstructive hypopneas as they occur. AutoSet adjusts in increments as small as 0.2 cm H2O to ensure that pressure increases only as much as is necessary.
For flow limitation, AutoSet calculates the shape of the inspiratory flow-time curve and the value for every breath (using a metric known as the flattening index); however, it responds based on the average value of the most recent five breaths, as described above. Detection of flow limitation enables the device to increase the pressure before obstruction occurs, making treatment preemptive, and thus reducing the number of respiratory events and arousals. The apnea response is determined by the severity of the event and current therapy pressure. Apnea pressure changes are delivered after the event such that the pressure change will not arouse the patient. Snore response is measured using the severity of the vibrations of the snore. A more severe snore will give a larger pressure response, but this proportional response is delivered over the next series of breaths such that the pressure change does not disturb the sleeping patient.
If no further flow limitation, snore, or apneas are detected, therapy is reduced over time toward the minimum pressure prescribed by the physician with a 20-minute time constant. This approach allows the pressure from ResMed’s AutoSet algorithm to return to lower pressures for increased patient comfort in the absence of any respiratory events.
Philips Respironics: With its proactive and continuous analysis throughout the therapy session, the REMstar Auto algorithm has the unique ability to deliver just enough CPAP pressure necessary to ward off a potential event. Since the pressure delivered at any given time is slightly higher than the pressure level necessary to open the airway, if an event does occur, the device does not need to rapidly respond by increasing pressure quickly. When the REMstar Auto detects a clustering of events, it determines the patient’s airway to be unstable and slowly increases pressure to achieve a higher level of CPAP for a new 5-minute period.
The REMstar Auto detects and responds to apneas, hypopneas, flow limitations, and vibratory snores. To detect an apnea or hypopnea, the algorithm calculates a baseline patient flow based on a moving average of patient flow. The baseline flow and any changes in flow are based on the algorithm’s analysis of four parameters of the flow signal: flatness, roundness, peak, and shape. This precise recognition of unique patient flow patterns is the reason why the REMstar Auto reacts better than other devices.
Sleep Review: Finally, what was the basis or reference for incorporating the above-described approach to detecting and responding to sleep-disordered breathing events?
Fisher & Paykel: Flow-based algorithms have become industry standard due to the evidence supporting flow limitation as the most effective means to predict upper airway collapse (Ayappa, 1998). By using this well-established detection method in combination with SensAwake technology, the Fisher & Paykel SleepStyle 200 Auto is able to offer an effective treatment solution that addresses pressure intolerance that can adversely affect compliance.
DeVilbiss: The creation of the DeVilbiss IntelliPAP AutoAdjust algorithm was initiated in the early 1990s. The algorithm was first born based on several clinical resources and references, then grew through the utilization of a computer-assisted diagnostic algorithm to accurately define respiratory events. Finally, the AutoAdjust and its algorithm furthered evolved as a result of fine-tuning based on extensive real-world clinical testing.
ResMed: ResMed’s AutoSet algorithm was the first published auto-titration positive airway pressure algorithm in the peer-reviewed literature. The AutoSet was first developed in the early 1990s by researchers in Sydney, Australia, and Essen, Germany. Michael Berthon-Jones, MD, PhD, and Professor Helmut Teschler, MD, PhD, published a seminal article in the peer-reviewed literature (Thorax, 1998) comparing AutoSet versus continuous positive airway pressure. This study showed clinical equivalence of outcomes from AutoSet and CPAP in terms of respiratory disturbance index (RDI) and other important SDB parameters. Another important early analysis in the peer-reviewed press from the mid 1990s was published in the blue journal by Lloberes et al (Am J Respir Crit Care Med, 1996) showing equivalence of sleep architecture in terms of sleep efficiency, stage 1-2 sleep, slow-wave sleep, and REM sleep between AutoSet and CPAP using gold-standard PSG analyses.
Just a few of the many dozen other articles published on AutoSet in the last 15 years are summarized below:
- Improvement in compliance as well as quality-of-life parameters such as SF-36 Vitality Scores and mental health metrics for patients on AutoSet versus CPAP, when CPAP pressures are equal to or greater than 10 cm H2O (Massie et al. Am J Respir Crit Care Med, 2003)
- Superiority of AutoSet versus competitive APAP algorithms in studies completed by independent, non-industry-sponsored analyses (Farre et al. Am J Respir Crit Care Med, 2002)
- Equivalent clinical outcomes (AHI, oxygen saturation) as well as equivalent or superior quality-of-life (SF-36, FOSQ, EuroQOL) when AutoSet was compared to gold-standard CPAP (Am J Respir Crit Care Med, 2004)
- Economic and cost-effective use of AutoSet in the home setting for treating obstructive sleep apnea (Bachour et al. Sleep Medicine, 2007)
Literally millions of patients have been prescribed the AutoSet algorithm by physicians globally during the last decade, on products across product platforms from ResMed since the mid 1990s, including the AutoSet Clinical, the AutoSet Portable, the AutoSet P2+, the AutoSet T, and the S8 AutoSet. Today, patients can receive therapy from the latest AutoSet algorithm in the S8 AutoSet II device. The S8 AutoSet II device combines not only the advances of the world-pioneering auto-adjusting algorithm described in this article, but also one of the smallest, quietest, and most reliable sleep apnea devices in the world.
Philips Respironics: The theory of the algorithm was developed based on clinical understanding and practices used in titrating CPAP pressures during a PSG titration process. Additionally, there has been extensive clinical and bench test validation of the algorithm’s effectiveness. These studies have been conducted by Philips Respironics and independent medical professionals. Several studies have been published in medical and other trade journals.





{kind=link}