
Objective data provided by HST can optimize a dentist’s ability to titrate a mandibular advancement device. Titration HST results should not be shared directly with the patient, but should be passed on to the sleep physician prior to the follow-up sleep study.
An untuned guitar that arrives in the mail is useless until it is tuned to the proper pitch. If the strings are tightened too rapidly or too far, the neck will be strained and possibly damaged. Not enough string tension and the instrument will also not function properly.
Before the introduction of the modern electronic tuner, a guitarist had to rely only on trained ears to bring the instrument to the proper pitch. This new technology provided additional objective information that, when combined with the subjective sound of the instrument, led to ideal intonation of the guitar.
Likewise, an oral appliance can effectively open an airway during sleep only if it has been carefully advanced to its ideal three-dimensional position. That ideal position takes into account not only its effectiveness in achieving airway patency, but its suitability to the particular patient. In other words, it must be one the patient can tolerate on a nightly basis. But how does the dentist determine where that position is? Although it has been demonstrated that the degree of mandibular protrusion is generally correlated with increased device efficacy, this is not always the case. For some patients, excessive protrusion beyond an ideal position not only exacerbates unwanted side effects such as temporomandibular joint (TMJ) pain and tooth movement, it also can have a negative impact on airway patency.1 Like the guitar tuner, the additional objective information provided by home sleep testing (HST) can optimize the dentist’s ability to more effectively adjust the oral appliance.
Challenges in Appliance Adjustment
In the past, dentists providing oral appliance therapy were limited to adjustments based on the patient’s subjective symptoms. Traditionally, a patient’s sleepiness or a bed partner’s reports of snoring would lead a dentist (or the patient) to advance the protrusive adjustment of an appliance. If no protrusive setting provided the relief of subjective symptoms, the vertical dimension of the device was changed. Conversely, a dentist hearing reports of TMJ-related pain would be likely to pause or reduce the appliance’s settings until the patient was comfortable.
However, there are many clinical situations when a patient’s subjective symptoms are not always obvious or even obtainable. Consider, for example, the patient with moderate or even severe obstructive sleep apnea (OSA) but no significant daytime sleepiness. Perhaps they don’t snore or, if they do, have no bed partner to witness it. On what basis is the dentist to adjust their appliance?
While mandibular advancement devices (MADs) have been consistently demonstrated to be more effective in reducing objective measures of airway obstruction than inactive sham appliances, there have been documented cases of the placebo effect on subjective outcomes.2
This scenario might be illustrated by the patient who experiences complete relief of subjective complaints while using the appliance, yet the sleep physician reports that follow-up polysomnography (PSG) revealed it has not effectively reduced the apnea-hypopnea index (AHI) or oxygen desaturation. What can the dentist do to have a reasonable expectation that a future PSG would have a better result than the first?
Dentistry and Home Sleep Testing
Modern HST devices are relatively unobtrusive and simple for patients to use. Their data can be scored by computers in a matter of moments. These range from relatively simple and less expensive Type IV monitors that typically measure only one or two channels such as oxygen saturation and heart rate to more sophisticated Type III models that measure four or more channels and are similar or identical to those used by sleep labs.
Many HST devices provide both raw data and computer-scored interpretations of that data. While these computer-scored tests have been demonstrated to significantly correlate to those scored by trained sleep technologists,3,4 they are not considered diagnostic. However, they can provide the dentist with valuable insight during the adjustment period.
The use of HST for the adjustment of oral appliances is consistent with the American Academy of Dental Sleep Medicine (AADSM) guidelines for dental sleep medicine, which states, “the dentist may obtain objective data during an initial trial period to verify that the oral appliance effectively improves upper airway patency during sleep by enlarging the upper airway and/or decreasing upper airway collapsibility.”5 The AADSM guidelines do not specify what device(s) may be used to gather the objective data nor does it provide any guidelines or protocols for their use. As is the case with other new technologies (for example, aerial drones), the introduction of technology commonly precedes any regulations or guidelines on their use. HST use by dentists has already become commonplace, as evidenced by the proliferation of dental HST providers and the results of a recent “HST in the Dental Setting” survey done in conjunction with this article. This proliferation underscores the urgent need for more specific guidelines regarding the use of HST technology in the dental setting.
Although some dentists currently use various types of HST to screen patients for OSA, this practice is considered controversial and specifically contrary to American Academy of Sleep Medicine (AASM) and AADSM recommended practices. As Harold A. Smith, DDS, AADSM president, explains, “Sleep apnea is a chronic disease that is associated with an increased risk for other serious medical complications including hypertension, cardiovascular disease, stroke, and Type 2 diabetes, and it also raises the risk for workplace injuries and motor vehicle accidents. Therefore, patient health and public safety can be jeopardized—and healthcare professionals held liable—if sleep apnea is overlooked or misdiagnosed, or if the severity of the disease is underestimated. Dentists who order a home sleep apnea test to screen for a medical disease are exposing themselves to significant liability risks.”
As an additional word of caution, any dentists who are considering utilization of HST or any other medical testing in their practice should confirm that such testing is within the scope of their practice of dentistry as defined by their particular state’s laws and regulations. According to Patrick J. Monahan II, a Connecticut-based attorney who advises healthcare professionals in regulatory matters: “If a dentist orders home sleep testing or other medical tests in a state in which the state legislature or other controlling governmental body has determined such tests to be outside the dentist’s permissible scope of practice, or if there is doubt about whether the tests are in or outside the scope of dentistry, that dentist risks adverse action against his or her license, as well as the risk that the dentist’s professional liability insurer will deny coverage for any alleged negligence associated with such tests.”
Case Example
SG is a 66-year-old nonobese male who was diagnosed by his sleep physician with moderate OSA (AHI: 25 (3%), oxygen saturation nadir: 79%, 12% sleep time with oxygen saturation below 90%). His chief complaints upon presentation to the sleep lab were excessive daytime sleepiness (Epworth Sleepiness Score: 17) and loud snoring reported by his bed partner. His medical history was remarkable for hypertension, atrial fibrillation, and borderline Type 2 diabetes. He has had two minor and one major motor vehicle accidents within the past 2 years. He was prescribed a CPAP by his sleep physician but after several failed attempts asked for an alternative treatment for his condition. At this point, he was referred to our office for evaluation. Clinical and radiographic examination (a recent full series of dental x-rays) revealed no contraindications to oral appliance therapy.

A SomnoMed Herbst Advance has an 8 mm range and millimeter scales on each side that facilitate observation of the protrusive position.
A SomnoMed Herbst Advance appliance was fabricated at an initial protrusive position of 50% (6 mm out of 12 mm protrusive range). This particular appliance has an 8 mm range and millimeter scales on each side that facilitate observation of the protrusive position.
His starting position corresponded to the 1 mm marks on each side of the appliance, which allowed for 1 mm retrusive and 7 mm protrusive adjustments. He was instructed not to advance the appliance during the initial first week period. At 1 week post-insertion, he reported that he was feeling somewhat less sleepy. His wife reported that he was still snoring although not nearly as loudly. He had no dental or TMJ-related complaints and was meticulously following all postoperative instructions. He was instructed (verbal and printed) to advance the device 0.5 mm each week but only if he was not experiencing any TMJ pain and to continue to do so up to a maximum of 2 mm or until his sleepiness and snoring were resolved.
He returned for follow-up 4 weeks later, and he and his wife happily reported the sleepiness and snoring were effectively eliminated by the appliance. He reported he had advanced the appliance a total of 1 mm on both right and left sides. This was confirmed by observation of his appliance.
Subsequent follow-up visits over the next 2 months revealed no change in his subjective symptoms. This very happy patient was referred back to his sleep physician to evaluate the efficacy of the device.
Much to all of our surprise and disappointment, the report from his sleep physician indicated that his AHI was now 33 with the device in place and his oxygen desaturation nadir and duration essentially unchanged.
The patient was then instructed to further advance the appliance 0.5 mm per week (unless he had dental or TMJ-related symptoms) for a total of no more than 4 mm total. At this point, he had a total of 6 mm protrusive range from his current setting.
He was followed every 2 weeks during this time and showed no signs of difficulty with the advancement of his device.
After the appliance was advanced the full 4 mm, the patient was sent home with a Type III ResMed ApneaLink Air HST device, as well as additional AAA batteries for each night of use. His instructions (verbal and printed) were to use the monitor on each of 3 nights with the first night at the current appliance position and reduce the setting 1 mm on each subsequent night (see Figure 1). All patients who are to receive a HST from our office sign a written agreement that describes their specific responsibilities for any loss or damage to the device. The agreement also stipulates that the results of the test will not be shared with the patient, as doing so risks the possibility of implying a medical diagnosis.
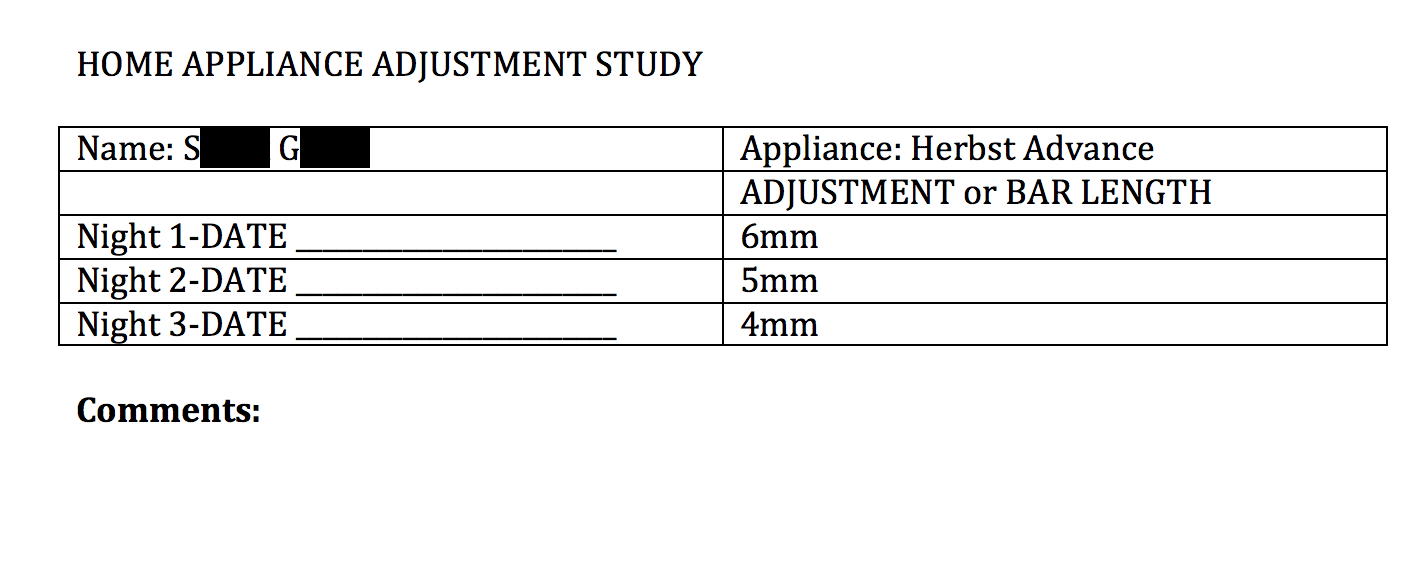
Figure 1. Home appliance adjustment study printed instructions given to patient.
The device’s data was downloaded and generated computer-scored results (see Figure 2).
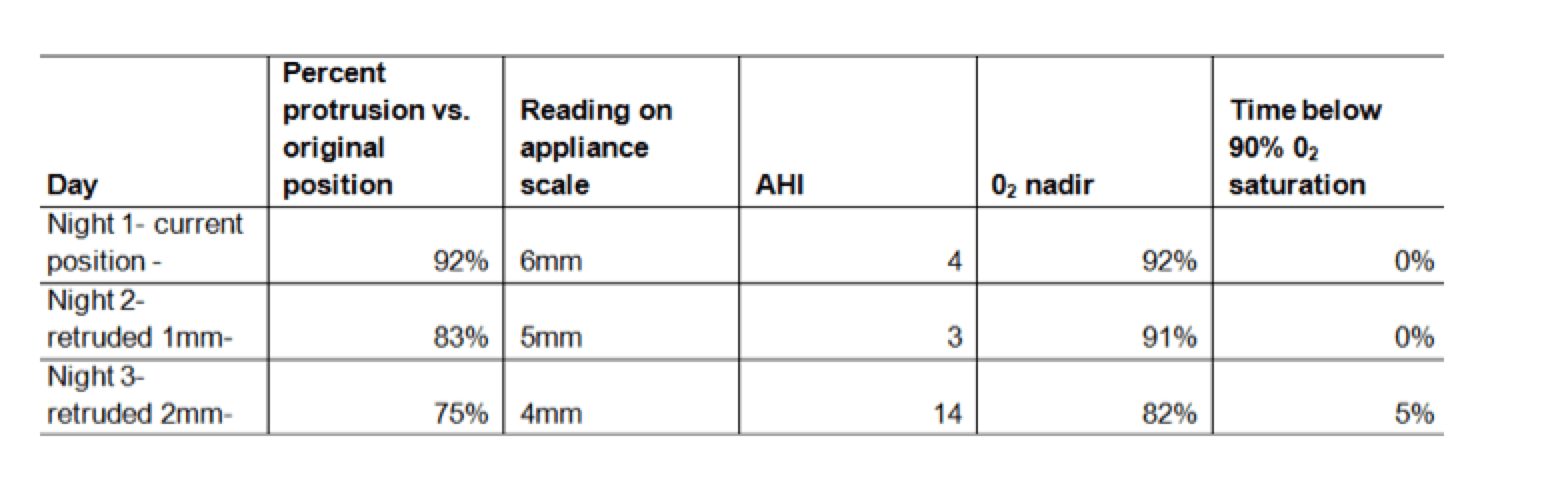
Figure 2. Patient’s computer-scored home appliance adjustment study results.
Based on the HST adjustment study results, the patient was instructed to keep his device at the 5 mm setting for the subsequent follow-up with his sleep physician. The results of the HST were not discussed with the patient (as was stipulated in the pretest signed agreement). Copies of the reports were forwarded to the patient’s sleep physician along with a link to retrieve the raw data.
The physician’s subsequent PSG 3 months later confirmed the efficacy of the device at the 5 mm position. The patient was scheduled for a 6-month follow-up appointment and asked to contact our office if there were any changes in his symptoms or issues with the appliance.
Discussion
Although symptomatic relief often corresponds with reduction in objective observations, this case confirms reports in the literature that this does not always hold true. The primary advantage of using multinight sleep studies versus the traditional practice of a single-night study at one appliance setting is the ability to retrieve the maximum amount of information in a relatively short amount of time. Although there are cost savings related to the reduced number of office visits and the ability to reuse disposable accessories during the 3 nights, they are offset by the potential expense of additional HST devices, each capable of recording at least 3 nights of data, that the patient retains for the longer testing periods.
Anthony T. Dioguardi, DMD, DABDSM
The protocol described in this article does have a notable disadvantage: HST is currently only approved for use by a physician for the diagnosis of OSA in patients with a high pretest probability of moderate to severe OSA. So a dentist, in collaboration with a physician, who is treating a patient with mild to moderate OSA—the type of patient who is more likely to be referred for oral appliance therapy than a patient with severe OSA—is gathering titration data in the range where HST reports are least reliable; that is, in cases of mild OSA. But in this author’s view, this disadvantage underscores my recommendation that these computer-scored tests, when used as described in this article, should not be shared with the patient. The titration HSTs are not diagnostic. However, the ability to share raw data from these tests with the sleep physician would certainly provide an avenue for more effective collaboration during the adjustment period.
In an ideal world, all follow-up MAD visits would be conducted jointly by the physician and dentist in the same physical location, with unlimited testing at no expense to the patient. But in reality, physician-administered HST assessments throughout the adjustment period would require additional patient travel and expense. Also, even the most generous insurance policies have a limit on how many tests will be covered. So the protocol described in this article is a real-world effort to incorporate this new technology to assist the dentist in establishing a tentative appliance setting prior to assessment by the sleep physician, in the absence of any specific published guidelines.
Today, there are many technological advances in sleep medicine that offer providers superior options to serve patients’ needs. HST in the dental setting, when used appropriately, is a tool that can increase a dentist’s ability to collaborate more efficiently and effectively as a partner in the treatment of sleep disorders.
Read a letter to the editor about this article, as well as Dioguardi’s reply.
Anthony T. Dioguardi, DMD, DABDSM, is a general dentist with extensive training and experience in the management of snoring and obstructive sleep apnea with oral appliances. As an active participant with Yale University’s Sleep Medicine post-doctorate fellowship program since 2009, he provides clinical and academic instruction in the dental treatment of sleep-disordered breathing. He is a member of Sleep Review’s editorial advisory board.
References
1. Remmers J, Charkhandeh S, Grosse J, et al. Remotely controlled mandibular protrusion during sleep predicts therapeutic success with oral appliances in patients with obstructive sleep apnea. Sleep. 2013;36(10):1517-25. doi:10.5665/sleep.3048.
2. Petri N, Svanholt P, Solow B, Wildschiødtz G, Winkel P. Mandibular advancement appliance for obstructive sleep apnoea: results of a randomised placebo controlled trial using parallel group design. J Sleep Res. 2008;17:221–29. doi: 10.1111/j.1365-2869.2008.00645.
3. Gantner D, Ge J-Y, Li L-H, et al. Diagnostic accuracy of a questionnaire and simple home monitoring device in detecting obstructive sleep apnoea in a Chinese population at high cardiovascular risk. Respirology. 2010;15:952–960. doi: 10.1111/j.1440-1843.2010.01797.x
4. Choi JH, Kim EJ, Kim YS, et al. Validation study of portable device for the diagnosis of obstructive sleep apnea according to the new AASM scoring criteria: Watch-PAT 100. Acta Otolaryngol. 2010;130(7):838–43.
5. AADSM Treatment Protocol: Oral Appliance Therapy for Sleep Disordered Breathing: An Update for 2013. www.aadsm.org/treatmentprotocol.aspx. Accessed June 6, 2016.





{kind=link}