The ‘CALMS’ framework introduces cognitive behavioral therapy principles to patients at any medical practice, while preserving the option of full CBT‑I later.
By Louise Berger
Insomnia is one of the most common conditions encountered across sleep medicine and general healthcare, yet many patients struggle to access effective treatment. Cognitive behavioral therapy for insomnia (CBT‑I) is a highly effective, first‑line intervention, but trained providers remain in short supply. As a result, many patients receive sleep hygiene advice or medication alone, approaches that rarely address the behavioral and cognitive processes that perpetuate chronic insomnia.
When access to effective care is delayed, insomnia often persists far longer than it needs to. Symptoms escalate, distress increases, and daytime functioning declines, even though earlier behavioral intervention could prevent much of this deterioration.

Many core components of CBT‑I, such as stabilizing routines, addressing conditioned arousal, reducing sleep‑related worry, and supporting circadian alignment, are already familiar to clinicians across disciplines. What is often missing is not the individual strategies but a clear structure and therapeutic stance for introducing them in a way that promotes adherence without increasing pressure or anxiety around sleep.
Across my clinical work and teaching, I have seen many patients wait months, sometimes years, before receiving CBT‑I. During this interval, the way insomnia is explained and managed can either preserve self‑efficacy and hope or inadvertently reinforce helplessness, sleep effort, and reliance on medication. Clinicians are left supporting patients without a clear framework.
I developed the CALMS framework to meet this need, offering clinicians from diverse backgrounds a clear structure for addressing the drivers of insomnia and introducing CBT‑I principles in a calm, collaborative way. Its purpose is to support earlier, safer, and more effective care within routine practice, while preserving the option for full CBT‑I when needed.
The CALMS Framework
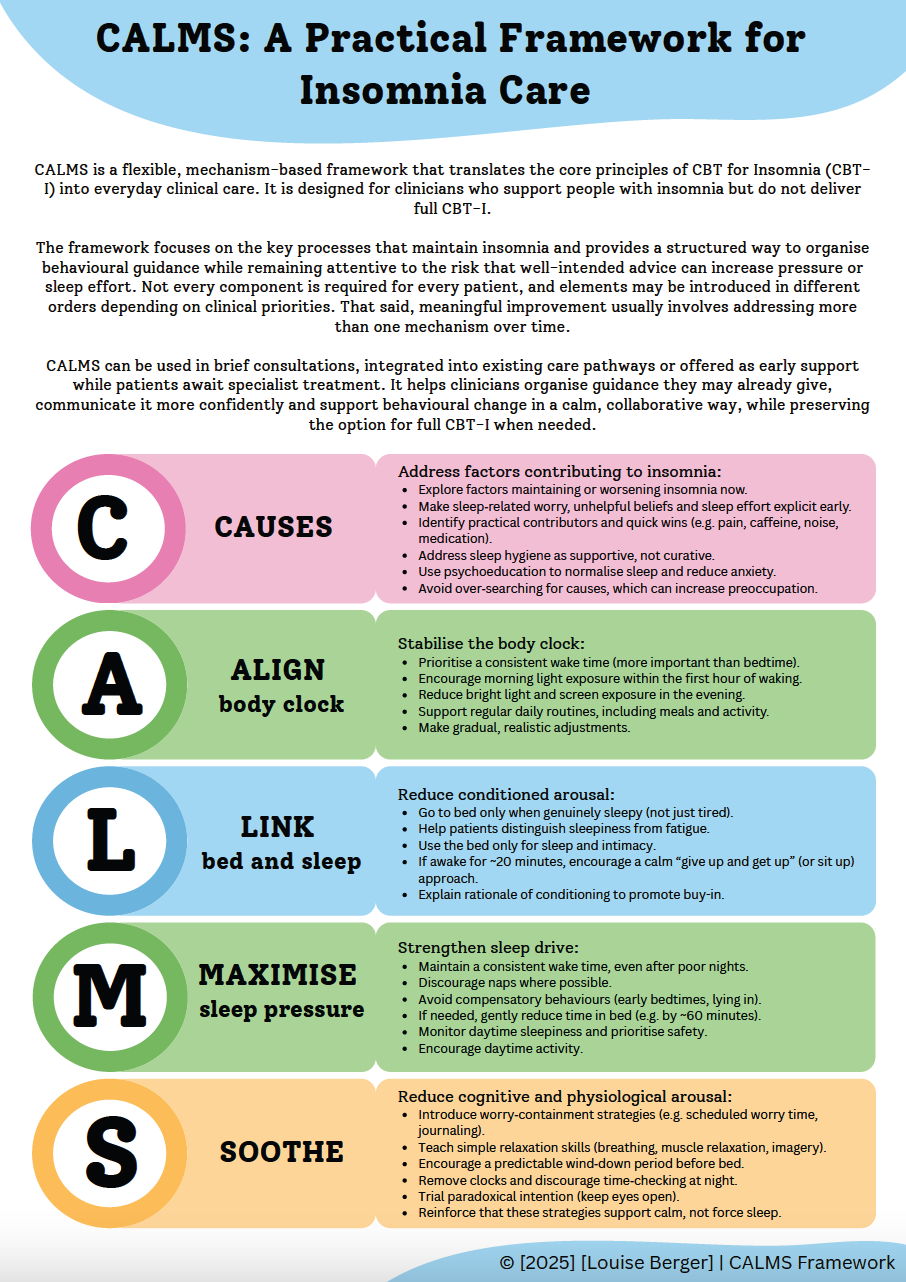
CALMS is designed as a flexible framework rather than a rigid sequence. Not every component is needed for every patient, and elements can be introduced in different orders depending on clinical priorities. The components work synergistically, and meaningful change usually involves addressing more than one mechanism over time.
Although CBT‑I strategies are most effective when applied consistently, their benefit can be reduced when guidance becomes a source of pressure or anxiety. CALMS therefore emphasizes flexibility and individualization, helping clinicians encourage helpful behavioral change without turning recommendations into rigid rules.
C = Causes
In CALMS, the “C” or “Causes” refers to any factor that may be driving, maintaining, or exacerbating insomnia and that can be usefully addressed at treatment outset. This includes the cognitive mechanisms that commonly perpetuate chronic insomnia, particularly worry, unhelpful beliefs, and sleep effort, as well as practical contributors such as pain, medication effects, environmental disruption, or excessive caffeine. The aim is not to identify a single cause, but to take a calm, pragmatic look for modifiable factors that may reduce arousal or exacerbate sleep difficulty and offer quick wins.
A key focus at this stage is helping both clinician and patient recognize the role of sleep‑related anxiety and effort. Sleep effort rarely responds to technique alone. It reduces when interventions are framed in ways that lower pressure, loosen rigid rules, and reduce self‑monitoring.
Without this understanding, even well‑intended behavioral strategies can inadvertently increase vigilance or urgency, reinforcing the very processes they are intended to change. Naming sleep effort early supports a therapeutic stance of flexibility, compassion, and collaboration that shapes subsequent steps.

Clinical Focus at the Causes Stage:
- Identify obvious, modifiable contributors that may increase arousal or exacerbate sleep difficulty.
- Offer targeted psychoeducation and perspective-shifting to address sleep myths and reduce sleep-related anxiety and catastrophic thinking.
- Frame sleep hygiene as supportive rather than curative.
- Emphasize that sleep cannot be forced and that reduced effort and preoccupation support recovery.
Not all contributing factors can be identified or modified, and excessive focus on “finding the cause” may itself increase sleep preoccupation. When no clear targets emerge, treatment proceeds through the remaining CALMS components, where the core behavioral mechanisms of insomnia are addressed directly.
A = Align Body Clock
Circadian rhythms play a central role in sleep regulation. Irregular wake times, poorly timed light exposure, and inconsistent daily routines can disrupt these rhythms, making it harder to fall asleep, stay asleep, or feel sleepy at the right times. Aligning the body clock provides a stable foundation for sleep and reduces the likelihood of nocturnal wakefulness.

Key Interventions at the Align Body Clock Stage:
- Set a consistent wake time, ideally aligned with the person’s chronotype. A stable wake time anchors the circadian system and supports more predictable sleep onset.
- Encourage morning light exposure within an hour of waking, such as a short walk or sitting outside with a coffee, to help shift the body clock earlier and consolidate the sleep-wake rhythm.
- Reduce evening light exposure by using dimmer lighting and lowering screen brightness in the hours before bed.
- Support consistent mealtimes and discourage late‑night eating, which can send conflicting time cues.
- Promote meaningful daytime activity and routine, strengthening environmental time cues that regulate circadian timing.
Prioritizing wake time as the primary anchor, rather than prescribing rigid bedtimes, can ease sleep effort and support a calmer relationship with sleep. Also, patients often find gradual adjustments to the sleep-wake timing easier to sustain.
L = Link Bed and Sleep
Conditioned arousal is a core perpetuating mechanism in chronic insomnia. Over time, repeated wakefulness in bed teaches the brain to associate the bed and bedroom with alertness rather than sleep. Patients often describe this as, “I’m nodding off downstairs, but the moment I get into bed, it’s like a switch flips.”
When the bed becomes a cue for wakefulness, even brief periods of lying awake can reinforce the pattern. Re‑establishing the bed as a cue for sleep is therefore a central component of treatment.

Key Interventions at the Link Bed and Sleep Stage:
- Go to bed only when genuinely sleepy, not just tired or “because it’s time.” Clinician prompt: Many patients conflate sleepiness with fatigue. Offer simple cues they can use, such as noticing heavy eyes, drifting attention, or the sense that sleep is imminent.
- Limit bed use to sleep and intimacy to strengthen the bed-sleep association.
- If awake for around 20 minutes, encourage a give-up-and-get-up approach: leave the bed, do something pleasant and relaxing in low light, and return only when sleepiness returns.
- For those with mobility limitations, use a give-up-and-sit-up alternative, such as engaging in a quiet, upright activity rather than lying down awake.
The purpose of this step is not to enforce rigid rules but to reduce struggle, lower arousal, and help the bed feel sleep‑compatible again. Patients often value a clear rationale for this step, together with support in planning and troubleshooting around getting up.
M = Maximize Sleep Pressure
Homeostatic sleep pressure, sometimes described as sleep appetite, builds gradually across the day and is essential for consolidated sleep at night. Excessive time in bed and common compensatory behaviors such as napping, going to bed early, sleeping in, or avoiding activity can weaken this process. Although these strategies are understandable responses to poor sleep and fatigue, they often reduce sleep pressure and increase the likelihood of prolonged wakefulness in bed.
Maximizing sleep pressure helps consolidate sleep, reduces time spent awake at night, and supports a more predictable sleep-wake rhythm.

Key Interventions at the Maximize Sleep Pressure Stage:
- Maintain a consistent wake time to preserve sleep pressure, avoiding sleeping in or naps (even after difficult nights) that dilute the drive for sleep.
- Encourage meaningful daytime activity and regular exercise to build natural sleep pressure.
- For individuals with low sleep efficiency, consider a modest reduction of time in bed (for example, 60 minutes) either through a later bedtime or earlier wake time to consolidate sleep. This gentler approach mirrors core CBT‑I principles while remaining suitable for non‑specialist settings.
CALMS does not use formal sleep restriction therapy, which requires specialist training. Instead, it applies a lighter‑touch consolidation approach to reduce wakefulness in bed while maintaining safety and flexibility. Always assess for daytime sleepiness (for example, using the Epworth Sleepiness Scale) and monitor closely in individuals with excessive sleepiness.
S = Soothe
Insomnia is characterized by heightened cognitive and physiological arousal that persists across the 24‑hour period. Effective intervention, therefore, focuses not on forcing sleep but on cultivating calmer days and reducing arousal, which in turn makes sleep more likely. The aim is to support a steadier baseline, not to induce sleep on demand.

Key Interventions at the Soothe Stage:
- Introduce simple cognitive strategies that reduce mental arousal, such as constructive worry, journaling, or setting aside a brief “thinking time” earlier in the day. These approaches help contain rumination and reduce the mental load carried into bedtime.
- Teach relaxation techniques such as progressive muscle relaxation, paced breathing, or visualization. Daytime practice helps build the skill, and at night, these techniques simply help the body become more receptive to sleep. Free apps (such as Insight Timer) can support learning and maintenance.
- Establish a buffer zone between essential tasks (work, chores) and bedtime. Encourage a predictable period of low‑stimulation activity—dim lights, reduced screens, calming routines—to signal the transition towards rest.
- Use paradoxical intention (that is, intentionally keeping the eyes open and staying awake) to reduce sleep‑related effort by shifting attention away from sleep.
- Remove or cover clocks and avoid checking the time at night, as this increases cognitive arousal and sleep‑related pressure.
Like exercise, relaxation is a skill that develops with regular practice. One session rarely produces lasting change. Its purpose is to reduce baseline arousal and support a calmer relationship with sleep, not to induce sleep directly. A gentle, flexible approach helps prevent these strategies from becoming another source of pressure or performance.
Bringing CALMS Into Practice
CALMS offers clinicians a practical way to introduce the core principles of insomnia treatment within routine care by focusing on the mechanisms that matter most: aligning circadian rhythms, strengthening the bed as a cue for sleep, building sleep pressure, and reducing sleep effort and preoccupation.
It does not require long appointments or specialist training. Even brief conversations can help patients understand their sleep more clearly and begin making meaningful adjustments. These elements can be woven into existing care pathways, used opportunistically in consultations, or offered as early support while patients wait for specialist treatment.
Even a single shift, a steadier wake time, a calmer transition to bed, or a reframed belief can begin to ease the cycle of chronic insomnia. Introduced early and without pressure, these changes can reduce struggle, restore confidence, and create momentum toward more stable sleep.
When symptoms are complex, safety concerns arise, or progress plateaus, referral to a trained CBT‑I provider remains essential.
A Practical Step Forward
Insomnia is common, persistent, and often overlooked, yet it responds powerfully to behavioral change when patients receive clear guidance with a rationale. CALMS gives clinicians a memorable, mechanism‑focused way to start those conversations without overpromising or stepping beyond their scope.
By helping patients understand their insomnia with less fear and more agency, CALMS supports small, achievable shifts that can turn nights and days that once felt like a battle into something calmer and more livable, while keeping the door open to full CBT‑I.





{kind=link}