 |
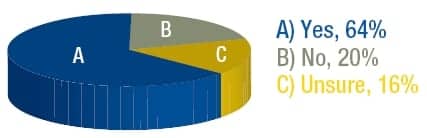
Support for pay-for-performance (P4P) programs exists, but implementation has been slow. According to a Sleep Review Web poll, 64% of readers support such programs. Organizations like the American Thoracic Society (ATS) also endorse P4P for sleep medicine, but there are a number of hurdles to overcome before adoption of these programs becomes more widespread. By keeping performance improvement and patient outcomes the central argument for implementation, advocates of P4P programs can maintain the momentum for support.
In late 2008, the American Academy of Sleep Medicine along with the AMA Physician Consortium for Performance Improvement (PCPI) developed performance measures for obstructive sleep apnea. These measures look at four areas: assessment of sleep symptoms, severity assessment at initial diagnosis, positive airway pressure (PAP) therapy prescribed, and adherence to PAP therapy.
“The way these measure sets work is that you are required to report every patient that you take care of with this diagnosis. At least 80% of patients in your panel that you care for with this diagnosis must meet these measures,” says Patrick J. Strollo, Jr, MD, FCCP, FAASM, cochair of the committee that developed the OSA Physician Performance Measurement Set. “And if you do, in the pay for performance legislation, then you would be subject to a small additional payment—1% to 2%.”
Financial incentives are alluring to physicians, but this has not kept such programs from criticism. While scientifically sound, the measures are not infallible. Obstacles include concerns about physician autonomy, the potential for patient cherry-picking, the problem of attribution (who is responsible for reporting various measures), consequences that may occur to a physician practice as a result of adopting performance measures, and lack of electronic medical record (EMR) adoption.
“The pay-for-performance initiative has been piloted in a couple of areas, but it has not been embraced as enthusiastically as many people thought,” says Strollo. “The barriers are usually related to not having an electronic medical record.”
|
| WEB POLL: The American Thoracic Society recently endorsed pay-for-performance (P4P) for pulmonary, critical care, and sleep medicine. Do you support P4P programs? |
P4P hurdles have not gone unnoticed. For example, the government has introduced incentives in hopes of sparking physician implementation of EMRs.
As of now, the OSA measurement set has not yet been included by CMS as one of the PCPI measures. While the kinks are being worked out, keeping the focus on patient care will help to garner support of physician groups and the endorsement of individual practitioners. “Performance improvement must remain the central tenet of P4P, and performance is defined by the degree to which these initiatives promote the delivery of high-quality patient care,” said former ATS President John E. Heffner, MD.
Strollo echoes these comments. “Quite frankly, there is a very good argument to be made that when you standardize care, you decrease variability. Ultimately, what we’re interested in is improving patient outcomes.”
—Franklin A. Holman
[email protected]




