
A Sleep Severity Index that combines symptom count and symptom intensity aims to give dentists and other clinicians a clearer, more actionable picture of sleep-disordered breathing in children.
By Earl Bergersen, DDS, MSD, ABO
Sleep questionnaires are a reliable indicator of abnormal sleep issues in children, but they don’t simultaneously take into account both the number and severity of symptoms. Based on a questionnaire I published in 2015, I have recently developed a new Sleep Severity Index to be an easy, informative analysis for sleep problems, primarily for use in children, that provides five grades that incorporate symptom number and symptom severity. I believe this new index will be a reliable tool for dentists and other healthcare professionals.
What Prior Pediatric Sleep Questionnaires Have Shown
Several analyses of abnormal sleep in children have been developed to assess the presence and intensity of various sleep-disordered breathing symptoms.
- Spuryt et al analyzed 27 questions, such as loudness of snoring and apnea, together with their levels of severity, and found that certain questions are useful in identifying sleep-disordered breathing in children.
- The 22-question Pediatric Sleep Questionnaire indicates a threefold increased risk of obstructive sleep apnea (OSA) and identifies 14 behavioral symptoms related to snoring, sleepiness, and behavior.
- Some studies analyze questionnaire effectiveness, as well as pediatric measures of sleep issues, establishing parameters of sleep disturbances.
- Various investigations of sleep questionnaires have made recommendations, categorized them, and evaluated their reliability.
Study Population Used to Develop the Sleep Severity Index
I analyzed data from 1,034 nontreated children with a mean age of 7.9 years to develop the Sleep Severity Index. There were 551 males and 483 females. With no significant difference between them, the sexes were pooled.
Sample Size: 1,034
Mean Age: 7.9 years
Males: 551 (53.3%)
Females: 483 (46.7%)
Ethnicity (Estimated due to only 68% indicating their ethnicity):
Caucasian: 87.5%
Latino: 5.0%
Asian: 4.5%
African-American: 2.4%
Other: 0.4%
The severity of each symptom was indicated as:
- 0 (not present),
- 1-2 (mild),
- 3 (moderate),
- and 4-5 (pronounced).
The mean number of symptoms present per child was 8.6, and the total severity of these symptoms was 21.4—resulting in a mean Index of 30.
# Symptoms / Case: 8.6
Mean Severity / Case: 21.4
Mean Index / Case: 30.0
Incidence:
2-3 years: 2.6%
4-6 years: 25.7%
7-9 years: 46.5%
10-12 years: 22.1%
13 years: 3.1%
Statistics were used to determine differences (“t” test). The confidence interval was used at 95% for prediction purposes. The level of confidence (p) was considered significant at p=0.05.
Defining the Sleep Severity Index Grades
The sample was divided into five grades of severity termed the Sleep Severity Index.
Thirteen columns from A to M explain the elements that result in the 5 grades of the index. This chart is separated into three sectors:
- the impact of the symptoms (columns A to D),
- the severity of the symptoms (E and F),
- and the index (G to M).
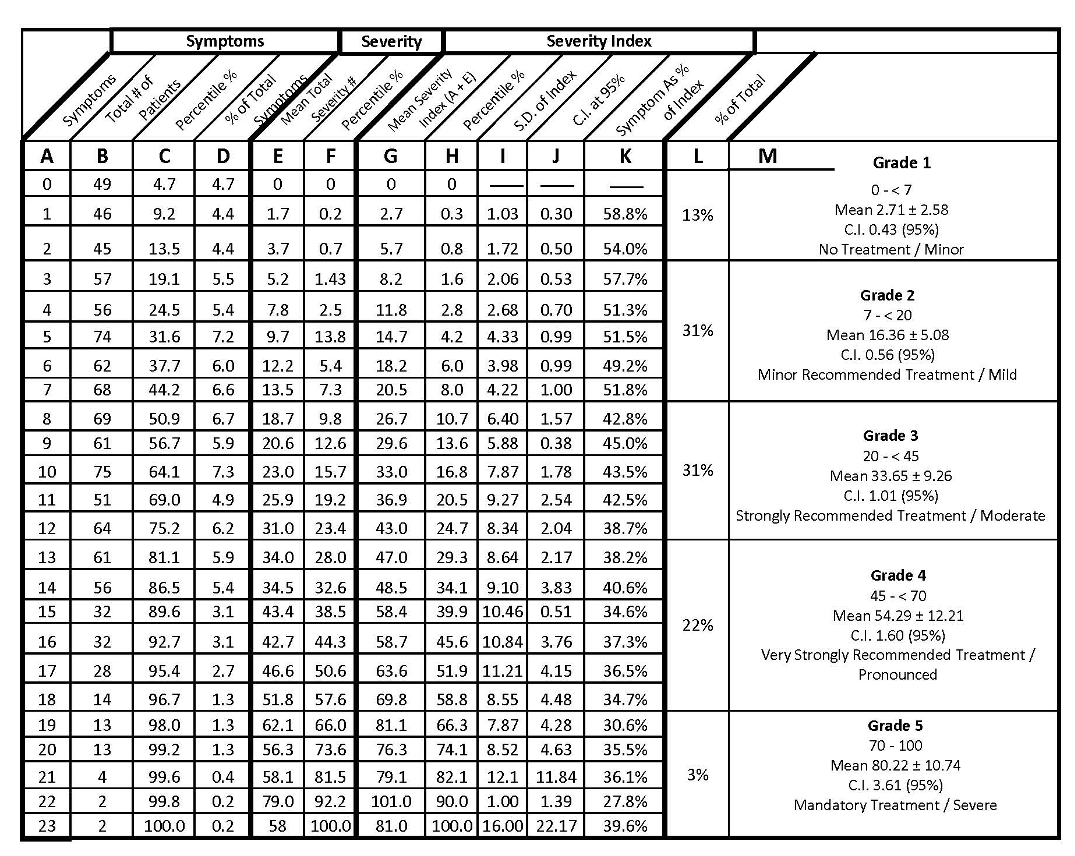
Those individuals with a severity rated as 0 on a sleep questionnaire have no symptoms present. Grades 1 and 2 are considered to be minor and mild. Grade 3 is moderate, and Grades 4 and 5 are pronounced and severe.
From column L, it can be observed that 87% of children (Grades 2-5) are basically in need of treatment of sleep-disordered breathing, while 56% (Grades 3-5) are in substantial treatment need, while only 13% are not recommended for treatment.
The mean number of symptoms per patient being 8.6, and the severity of 21.4 is in close agreement with an earlier article I co-authored.
Often, a diagnosis of a patient with abnormal breathing issues is determined only by the number of symptoms present, while ignoring the individual severity of these same symptoms. When one considers the number of symptoms together with their severities, a more complete analysis results.
A reduction of symptom influence from Grade 1 of a mean percent of the index amount of 56.4% (column K), down 40% to a mean percent at Grade 5 of 33.9%. In other words, as the index grades increase from Grade 1 to Grade 5, the influence of the symptom occurrence decreases while the severity of these same symptoms increases. This greater increase increment of severity over the number of symptoms present is also observable in column K.
One can observe the percentage decrease of the symptom influence on the index from 58.8% at Grade 1 to as low as 27.8% at Grade 5.
Grades 2, 3, 4, and 5 represent 87% of the total sample. The index range from Grade 1 is from 0 up to 7, with a mean of 2.71± 2.58. The confidence interval at 95% is 0.43. The table shows the mean number of symptoms (column A), their severities (column E), and index (column G) for the five grades of severity.
Another comparison indicates the increase of the symptoms present increases from grade 1 to 5 from 1 to 23 (column A) while severity increases from 1.7 to 79.0 (column E), which is 3.4 times more. As a result, since a Sleep Severity Index incorporates both of these variables by adding them together, for which the total represents the Sleep Severity Index (column M), a more precise analysis.
How the Index Prioritizes Clinically Meaningful Symptoms
It is important to relay the information on the Sleep Severity Index to the parent. Some symptoms, such as apnea, are more important than others, such as hypopnea, according to most research, even though apnea is not often present in young children (an incidence of about 1% to 3%). Another symptom that is very important to a child is bedwetting. Since it is often embarrassing to the patient, bedwetting should be corrected even though it might be the only symptom present. The most common symptom is nighttime mouth breathing, which is present in about 69% of children.
In formulating a practical Severity Sleep Index, various principles were considered, including:
- important symptoms that take precedence and are recommended for treatment, even when present as a single occurring entity, are as follows: labored breathing, suspected apnea, nighttime mouth breathing, moderate and pronounced snoring with a severity of 3, 4 and 5, restless sleep, waking up at night, talking or walking in sleep, and the presence of bedwetting;
- any child with 3 other minor symptoms than those listed immediately above; and
- children with no symptoms present would not be recommended for treatment and are designated as Grade 1.
The advantage of the Sleep Severity Index is it can be adapted to any type of analysis, whether as a result of a parental questionnaire or to a more accurate analysis that can objectively measure mouth breathing, snoring, apnea, hypopnea, oxygen desaturation, increased thoracic effort, abnormal nasal breathing, and bruxism—as long as both the symptom and their severities can be identified. Regardless of how many symptoms are considered or their individual severity amounts, the same degrees of index grades can be established to provide an informative method of assessing a patient’s abnormal sleep.
Although the index is applicable for children, a similar Index technique can be applicable for any age group.
Why Severity Should Not Be Ignored in Sleep Screening

In my study of 1,034 children, I draw the following conclusions:
- The severity of the symptoms is more influential than the symptoms themselves (p=0.001),
- Recommendations for treatment account for 56% of the sample, while minor treatment is represented by 31%. No treatment is recommended for 13%.
- The mean number of symptoms per child varies from 1.0 (Grade 1) to 23.0 (Grade 5), with the mean being 8.6 symptoms per child in the total sample, while the mean severity is 21.4.
- The mean Severity Index per patient is 30.0 from the sample.
Role of Objective Sleep Testing in Refining the Index
Various data collecting instruments could help in providing more objective information, particularly in-lab and home night studies would help in obtaining more objective data on several symptoms. These symptoms are oxygen desaturations, apnea, hypopnea, snoring, mouth breathing, abnormal nasal breathing, thoracic effort, bruxism, stages of sleep, and leg movements. The data could be more accurate if it were only collected from the same clinic by the same investigator.
This study, however, is a good representation of average dental professionals as it was collected at the present time. As the dental profession becomes better equipped with current objective diagnostic equipment, the accuracy of the data would improve.
We recommend for you:
ID 278598776 | Child Checklist © Yuri Arcurs | Dreamstime.com




{kind=link}