
Clinicians are now recognizing sleep-related manifestations of long COVID. A sleep specialist sees a coronavirus infection as the only precipitant of RBD in a 69-year-old patient.
By Jeffrey McGovern, MD, FAASM, FCCP
A minority of patients infected with the COVID-19 virus develop “long COVID”—health problems linked to their infection that persist beyond four weeks. The World Health Organization has called for a multidisciplinary approach to supporting these patients.1
The case of a 69-year-old male who presented with rapid eye movement (REM) sleep behavior disorder following a COVID infection highlights the importance of recognizing other manifestations of long COVID, especially in regards to sleep medicine.
REM Sleep Behavior Disorder Characteristics
REM sleep behavior disorder (RBD) is characterized by abnormal behaviors emerging during stage R sleep that may cause injury or sleep disruption. RBD is also associated with electromyography (EMG) abnormalities during REM sleep. The EMG demonstrates an excess of muscle tone and/or an excess of phasic EMG twitch activity during REM sleep.2
Numerous clinical conditions, medications, and other risk factors can trigger RBD. The main clinical concerns of RBD rest with safety of the patient and bedmate, as well as development of neurodegenerative disease.
Case Report of RBD After COVID Infection
The 69-year-old male with a history of obstructive sleep apnea (OSA) and coronary disease with revascularization and stenting presented with increased hypersomnia. For more than 5 years, he has consistently used a non-recalled positive airway pressure machine set at 15 cmH2O. His most recent compliance report documented usage at 9 hours 38 minutes with apnea-hypopnea index (AHI) of 0.9 and no leaking. He underwent a recent cardiac catheterization showing patent stents and successful revascularization.
At the sleep evaluation, he mentioned his infection with COVID-19 (despite two doses of Pfizer-BioNTech vaccines), for which he had not sought outpatient or inpatient medical attention. In the same month after contracting COVID, he experienced nightly violent dreams and his spouse reported that he screamed and kicked during sleep. There was no report of injury to the bedmate, nor was there sleepwalking, restless legs, or change in medications.
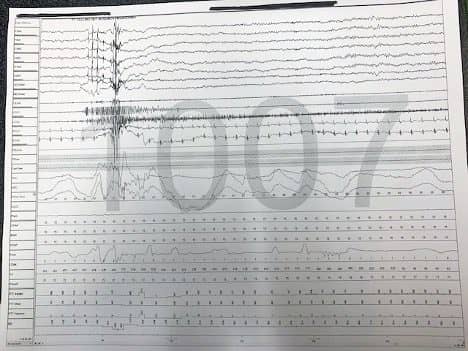
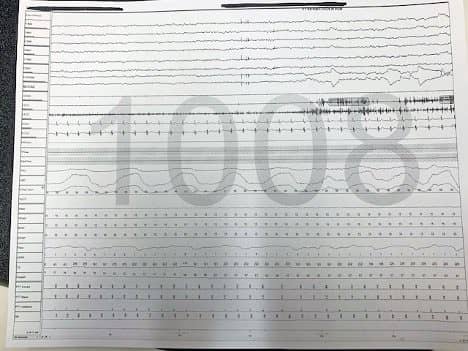
The patient underwent a retitration study in the laboratory because of the parasomnias. The study was manually scored using Respironics software (G3 version 3.9.0) in accordance with the American Academy of Sleep Medicine Manual and Associated Events: Rules, Terminology, Technical Specifications (version 2.6).3 The study demonstrated reduced sleep efficiency of 61.3%. Sleep was fragmented with increased N2 (71.1%) and reduced stage R (12.9%). Limb movement index (number/hour) was 118.8, which occurred in both REM and non rapid eye movement (NREM) sleep.
CPAP therapy was initiated at his current setting and remained at 15 cmH2O with AHI of 0.6 events per hour. The patient had an episode of yelling during stage R and recalled one of his typical, violent dreams during that time.
Upon review of the study with the patient, the patient acknowledged the violent nature of his dreams and the nocturnal movements witnessed by his bedmate since his COVID infection. He denied any tremors or gait abnormalities. He denied any recent trauma or new medications. He reported residual hypersomnia despite CPAP compliance.
I reviewed a safety plan for both him and his spouse and initiated clonazepam 0.5 mg at night. I ordered a no-contrasted magnetic resonance imaging (MRI) for medical reasons, which showed nonspecific hyper intense foci, mostly in supratentorial regions but with scattered foci in the pontine region. In a two week follow-up he noted reduction of his nocturnal events and hypersomnia. A neurology consult is pending.
Sleep Medicine Context
There are numerous published reports of multisystem involvement with COVID-19 but only recent reports in sleep medicine.4-6 In addition, the literature both nationally and internationally is only beginning to report on long COVID. Most centers with programs for long COVID are providing frameworks for research but the call for an infrastructure for rigorous research conducted alongside clinical care appears to be growing.7
There is no previous report of RBD associated with COVID-19. Whether this phenomenon may be seen as a more frequent long COVID sequela is yet to be determined. There is no other precipitant of REM parasomnia in this patient, and he has no other long COVID manifestations. While the MRI does show nonspecific hyper intense foci in the pontine region, there are more foci in the nonpontine regions.
The typical clinical symptoms in long COVID are tiredness, dyspnea, fatigue, brain fog, autonomic dysfunction, headache, persistent loss of smell or taste, cough, depression, low grade fevers, palpitations, dizziness, and muscle and joint pains.8 Brain fogginess appears to be particularly debilitating but the etiology of this symptom is not well elucidated. Researchers at Oxford University’s Wellcome Centre for Integrative Neuroimaging reported that participants several months after COVID-19 infection had more grey matter loss and tissue abnormalities than controls.9
Potential mechanisms by which the virus can alter brain structure proposed by the authors include reduced sensory input related to loss of smell, neuroinflammation or immune reactions, or direct viral infection of brain cells. Limitations of this study include reduced vaccination status and a population of only white, middle-aged males. Nevertheless, the documentation of altered brain regions is provocative.
Although the RBD patient’s symptoms are better controlled with clonazepam and he is now able to sleep safely with his bedmate, questions remain in regards to the manifestation of neurodegenerative disease that may be a fearsome sequela of this parasomnia. He will require indefinite neurologic follow-up. While there is no direction in regards to stopping the clonazepam, it is safer given his violent behavior to continue the clonazepam for now. It is not clear if there will be spontaneous resolution. He will continue to use his CPAP, which he has continued faithfully since the initiation of this therapy.
Role of the Sleep Specialist
This case highlights the manifestation of RBD in a patient with COVID-19 infection. Given the endemic nature of this disease and its myriad manifestations in long COVID, this case is important to report.
The sleep specialist plays an important role in the care of the medical and surgical patient and becomes an especially important contributor in the patient with REM parasomnia following COVID-19.
Jeffrey McGovern, MD, FAASM, FCCP, is director of the Allegheny Health Network (AHN) Saint Vincent Hospital Sleep Center. He is part of the multidisciplinary team at the AHN Post-COVID-19 Recovery Clinic. The author reports no conflict of interest.
References
- Rajan S, Khunti K, Alwan N, et al. In the wake of a pandemic: preparing for long COVID. World Health Organization. Policy brief 33. 2021.
- American Academy of Sleep Medicine. International Classification of Sleep Disorders, 3rd ed. 2014.
- Berry RB, Quam SF, Abreu AR, et al; for the American Academy of Sleep Medicine. The AASM Manual for Scoring Sleep and Associated Events. Version 2.6. 2020.
- Bryson WJ. Circadian rhythm sleep-wake disorders and the COVID-19 pandemic. J Clin Sleep Med. 2020 Aug 15;16(8):1423.
- Salles C, Mascarenhas Barbosa H. COVID-19 and obstructive sleep apnea. J Clin Sleep Med. 2020 Sep 15;16(9):1647.
- Genta FD, Rodrigues Neto GB, et al. COVID-19 pandemic impact on sleep habits, chronotype, and health-related quality of life among high school students: a longitudinal study. J Clin Sleep Med. 2021 Jul 1;17(7):1371-7.
- Parker AM, Brigham E, Connolly B, et al. Addressing the post-acute sequelae of SARS-CoV-2 infection: a multidisciplinary model of care. Lancet Respir Med. 2021 Nov;9(11):1328-41.
- Halpin S, O’Connor R, Sivan M. Long COVID and chronic COVID syndromes. J Med Virol. 2021 Mar;93(3):1242-3.
- Douaud G, Lee S, Alfaro-Almagro F, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022 Apr;604(7907):697-707.
Photo 181168877 © Wave Break Media Ltd | Dreamstime.com





{kind=link}