
A sleep center shares its sleep technologist-driven flow chart to increase the likelihood of successful titration for patients with Cheyne-Stokes breathing, treatment-emergent central sleep apnea, and opiate-induced central sleep apnea.
Sleep-disordered breathing (SDB) is defined as the repetitive cessation or decrease of airflow during sleep and encompasses both obstructive sleep apnea (OSA), characterized by occlusion of the airway with continued effort to breathe, and central sleep apnea (CSA), characterized by the absence of respiratory drive to breathe and absence of respiratory effort on the polysomnogram (PSG). Whereas OSA is quite common, CSA comprises a small percentage of patients referred to the sleep laboratory and accounts for about 5% to 10% of patients with SDB.1 Though the treatment of OSA with positive airway pressure (PAP) therapy is relatively straightforward with well-defined protocols, treatment protocols for CSA are less well established. In the sleep laboratory, the technologist is tasked with initiating therapy for both types of sleep apnea and determining an optimal treatment level.
At our sleep laboratory at the University of Kansas Health System, we have utilized a number of suggested protocols and have had varying success in the use of PAP in treating CSA in a split-night protocol. We contacted several sleep laboratories in our region and found no consensus on a PAP titration protocol for CSA; in some sleep labs, a written protocol did not even exist. Our goals were to better understand characteristics of CSA, review the literature related to using PAP therapy in the treatment of CSA, and develop a more effective titration protocol.
CSA does not have a single cause. So, should there be a one-fits-all titration protocol?
CSA can be primary (idiopathic) or secondary to other conditions including heart failure, stroke, central nervous system suppressant drugs, and kidney failure. Primary (idiopathic) is considered to be a rare disorder, occurring more frequently in middle-aged to elderly individuals and is the least common form of CSA encountered in the sleep lab.2
Cheyne-Stokes breathing (CSB) is a unique form of CSA characterized by a crescendo-decrescendo pattern of breathing with a central apnea or hypopnea at the nadir of the ventilatory effort. CSB is typically associated with heart failure, but it can also occur in association with neurological disorders, including stroke, neurovascular disorders, and dementia. CSB is the most frequently encountered form of CSA identified during the baseline PSG and occurs in 44% of heart failure patients with reduced ejection fraction and 27% of heart failure patients with normal ejection fraction.1
Some patients with OSA develop central sleep apnea during CPAP titration. This condition is referred to as treatment-emergent central sleep apnea (TECSA), formally referred to as complex sleep apnea. TECSA occurs in patients with predominately obstructive sleep apnea during the baseline portion of the study with CSA emerging and predominating while on CPAP. This type of CSA occurs in 10% to 15% of the sleep center population.1 There appears to be increased incidence of TECSA in patients undergoing a split-night study, which may relate to factors including titration dynamics (such as higher pressures or a faster rate of pressure increase) or to underlying physiology as patients undergoing a split-night study may have more severe OSA.3 Other potential mechanisms for TECSA are mask leaks, narcotic use, central apneas pre-CPAP, and heart failure.
Finally, patients presenting with CSA due to chronic opioid use have been increasing due to increasing use of opiate pain medications. The frequency of patients exhibiting CSA in any given sleep center is highly dependent on the referral pattern for that center.
The detrimental effects of CSA include recurrent hypoxemia, non-restorative sleep, excessive daytime sleepiness, fatigue, and cognitive dysfunction. These are identical to those associated with OSA, and it may be difficult to distinguish between the two on a clinical basis. In addition, central and obstructive apneas may exist together in patients with heart failure and chronic opioid use. So, when the patient presents in the clinic, CSA is rarely the suspected diagnosis. Compounding the problem is the increasing prevalence of home sleep apnea testing (HSAT). The majority of devices used in HSAT studies have not been validated in detecting central apneas. So, the preferred diagnostic approach for patients with CSA is in-lab PSG.
In the sleep laboratory, it is critical the technologist be able to differentiate between obstructive and central events to appropriately choose a treatment pathway. In both cases, the typical course of action by the technologist is to institute PAP therapy for moderate to severe sleep apnea. Central sleep apnea is defined as a central apnea index (CAI) of ? 5 central apneas and/or central hypopneas per hour of sleep and the number of central apneas and/or central hypopneas is > 50% of the total number of apneas and hypopneas. Cheyne-Stokes breathing requires ? 5 central apneas and/or central hypopneas per hour of sleep and at least 3 consecutive apneas/hypopneas separated by crescendo-decrescendo breathing with a cycle length of at least 40 seconds and the number of central events is > 50% of total events.2 What makes the determination of CSA a little more difficult is the majority of sleep laboratories do not score hypopneas as being obstructive or central in origin and typically treat hypopneas as obstructive in nature, likely underestimating the occurrence of CSA.
Published PAP titration protocols for CSA have included use of the range of PAP therapies including CPAP, bilevel PAP (BPAP), and adaptive servoventilation (ASV) with ASV emerging as the therapy of choice. Studies have shown improved effectiveness of ASV over both CPAP and BPAP with lower AHI and improved compliance.4 However, the 2015 report related to the SERVE-HF study showing an increase in mortality in patients treated with ASV therapy who had an ejection fraction of ? 45% prompted the recommendation that ASV not be used in this subset of the population. Subsequently the American Academy of Sleep Medicine (AASM) revised its 2012 practice parameter for the treatment of CSA against the use of ASV in heart failure patients with EF ? 45% and moderate to severe sleep apnea.5 BPAP with a backup rate in these patients should be used with caution as the mechanism of effect is similar to ASV and there is little outcomes data to show effectiveness.6
To better understand how to approach PAP treatment of CSA, knowledge of the mechanisms of central apneas in each type of CSA is helpful. In general, CSA can be categorized as hypercapnic or nonhypercapnic.7 Hypercapnic CSA typically involves disorders associated with hypoventilation and is usually treated with PAP therapy to augment ventilation and was not included in our CSA protocol. In nonhypercapnic CSA, two physiologic phenomena are common: there is normal or slightly lower awake steady-state PaCO2 and increased ventilatory responsiveness to PaCO2 or hypoxemia (increased loop gain). In the situation of disrupted sleep (increased arousals), central events are perpetuated. Both CSB and TECSA fall into this category, and CSA due to opiates can have elements of both types. In patients with heart failure, CSB is believed to result from a high-gain ventilatory control system (increased hypercapnic responsiveness) combined with a prolonged circulatory time leading to unstable ventilatory control.

Robert Whitman, PhD, DABSM, RRT, RPFT
Based on a literature review, we approached development of our PAP titration protocol for treating CSA on the particular presentation as either CSB, opiate-induced, or TECSA. CPAP therapy is recommended as the initial treatment option for all types of CSA based on the premise that an obstructive component is usually present. In a study involving 162 patients with predominately CSA on diagnostic study, 50% were successfully treated with CPAP (success defined as CAI ? 5/h and an AHI < 10/h).8 When supplemental oxygen was added in the remaining patients, an additional 35% were optimally treated regardless of the etiology of CSA. In addition, 54% of patients on opioid therapy responded to CPAP and another 27% responded when O2 was added to maintain SaO2 ? 93% with the mean time from initiation of O2 to resolution of CSA of 78 minutes. Concomitant OSA was present in 98% of patients. The authors theorized the therapeutic effects of CPAP were due to restoring upper airway patency and stabilizing of respiratory control by increasing lung volume and oxygen stores. The optimal response to O2 in patients sub-optimally treated with CPAP was interpreted as due to a central stimulatory effect.
The development of TECSA may be related to unstable sleep states.2 That is, it depends on the combination of breathing instability, changes in upper airway related resistance, variable PaCO2 levels, and oscillating sleep state. Some patients may have tighter apnea threshold to hyperpnea response making them more susceptible to periodic breathing. Frequent arousals may lead to unstable sleep and oscillation of PaCO2. Mask leaks or mouth breathing during PAP titration may lead to hypocapnia, triggering central apneas. The presence of other medical comorbidities may also predispose certain patients to TECSA.
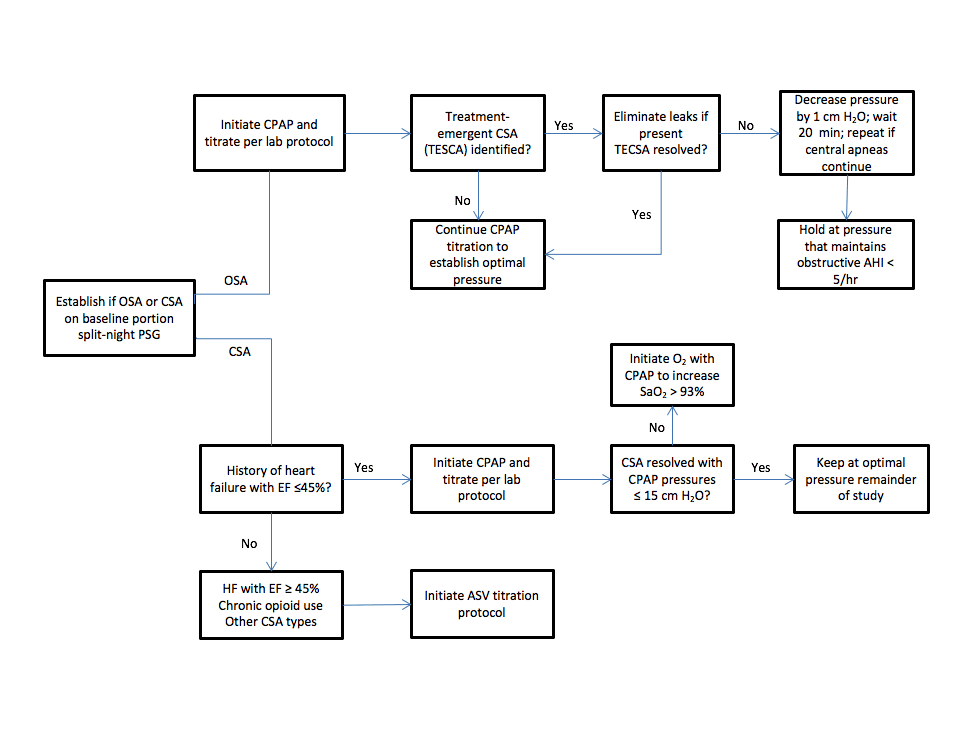
Figure 1. PAP titration protocol for central sleep apnea utilized at the University of Kansas Health System. (Click on image to make it larger.)
Our goal was to develop a CSA titration protocol for our laboratory and patient population that was technologist-driven, but consistently applied to result in the best likelihood of a successful titration (Figure 1). We based our protocol on key premises from the literature and AASM Practice Parameters:
- Primary CSA is not included in titration protocol due to low frequency encountered in the sleep laboratory.
- CPAP therapy is highly effective in CSB with an additional response to oxygen therapy in patients with sub-optimal response to CPAP.
- ASV therapy should not be considered in heart failure patients with an EF ? 45%.
- There is a high likelihood TECSA will resolve on CPAP therapy over time.
- PAP titration during a split-night study should allow for a slower titration rate and resolution of leaks to increase likelihood of success and not over-titrate.
- ASV therapy is the best option in patients with predominate CSA on baseline including heart failure patients with an EF ? 45% and patients with chronic opioid use.
- ASV is better than BPAP in therapeutic efficacy.
Our protocol is based on a split-night study. Patients returning for a second night PAP titration subsequent to a full-night baseline usually return with a physician-driven titration protocol prescription. Although sleep position can be effective in resolving CSA, maintaining a non-supine position was not included in our split-night protocol as our primary objective is to establish PAP efficacy. However, any effects on the frequency of central events due to position are reported for consideration of positional therapy as an available treatment option. A thorough review of patient’s medical history is performed prior to PSG to identify if the patient has heart failure with EF ? 45% or is on chronic opioid use.
We continue to re-assess our CSA PAP titration protocol relative to new research, updated practice parameters, and ongoing experience in our laboratory to ensure we continue to maximize patient treatment outcomes.
Robert Whitman, PhD, DABSM, RRT, RPFT, is director of the sleep center at The University of Kansas Health System and a member of Sleep Review’s editorial advisory board.
References
1. Macrea M, Katz ES, Malhotra A. Central Sleep Apnea: Definitions, Pathophysiology, Genetics, and Epidemiology. In: Principles and Practices of Sleep Medicine. 6th ed. Kryger M, Roth T, Dement WC, eds. Philadelphia, PA: Elsevier; 2017:1049-58.
2. American Academy of Sleep Medicine. International Classification of Sleep Disorders. 3rd ed. 2014.
3. Javaheri S, Smith J, Chung E. The prevalence and natural history of complex sleep apnea. J Clin Sleep Med. 2009;5:205-11.
4. Aurora RN, Chowdhuri S, Ramar K, et al. The treatment of central sleep apnea syndromes in adults: practice parameters with an evidence-based literature review and meta-analysis. Sleep. 2012; 35:17-40.
5. Aurora RN, Bista SR, Casey KR, Chowdhuri S, et al. Updated adaptive servo-ventilation recommendations for the 2012 AASM guidelines: The treatment of central sleep apnea syndromes in adults: Practice parameters with an evidence-based literature review and meta-analyses. J Clin Sleep Med. 2016; 12:757-61.
6. Badr MS. Central sleep apnea: Treatment. In: UpToDate, Collop N (Ed), UpToDate, Waltham, MA, 2017.
7. Zinchuk AV, Thomas RJ. Central Sleep Apnea: Diagnosis and Management. In: Principles and Practices of Sleep Medicine. 6th ed. Kryger M, Roth T, Dement WC, eds. Philadelphia, PA: Elsevier; 2017:1059-75.
8. Chowdhuri S, Ghabsha A, Sinha P, Kadri M, Narula S, Badr S. Treatment of central sleep apnea in US veterans. J Clin Sleep Med. 2012;8:555-63.





{kind=link}
My husband is taking several drugs for PTSD to curb nightmares, restlessness, and other sleep related issues. He has been unable to tolerate his prescribed Cpap. He is allergic to the mask and breaks out in a red angry rash every where the mask touches his face. Also, he complaines of dry eyes and trouble with mask leaks. Every time he tries using the Cpap he wakes up in the morning complaining of being tired more than ever because of all the problems with the mask leaking and becoming unseated every time he moves during the night. Do you have any suggestions for a mask or treatment that may be more tolerable for him than the full face mask he has now. Also, He wakes up choking and coughing due to extremely dry mouth when using the Cpap
Sounds like he needs humidification with his CPAP. As much as I do not normally recommend, he could explore an oral device.
There is a company called Pad a cheek that makes cloth barriers that go between the skin and the seal of the CPAP mask. I have seen them but never used them in our lab so I can’t speak about how well they work but this could be a solution if the mask is irritating the skin. Add humidification or heated humidification if not already done.
As Don stated, an oral appliance may be helpful but is only recommended for mild to moderate apnea. Insurance reimbursement for oral appliances is also usually an issue.
Good Luck!
Very nice review. I would add a brief comment, CSA can also be due to altitude sickness.