The 45-year-old presenting with moderate OSA didn’t develop that airway overnight. The architecture for it was built in childhood.
By Brooke Quinn, MSc, RPSGT, CSSC
One evening during our bedtime routine, my son looked up from the bathroom sink and asked a question I wasn’t ready for.
“Why do I have to breathe through my nose?”
He’s six. We’d been working through some breathing exercises together, part of the ongoing airway health routine that became a fixture in our evenings after his journey through adenotonsillectomy, continued evaluation, and the kind of persistent, subtle mouth breathing that makes a sleep scientist’s ears perk up even at the dinner table.
I paused before answering. Not because I didn’t know the science—I’ve spent years inside it. But because the honest answer is one that most clinicians, and nearly all parents, were never systematically taught.
The nose isn’t just where air happens to pass through. Nasal breathing is load-bearing. It shapes how the face grows, how the airway develops, how the brain gets oxygen during sleep. Once you start looking at airway health through a developmental lens, tracing the trajectory rather than reacting to the endpoint, something uncomfortable comes into focus.

The Hidden Timeline
In sleep medicine, we’re very good at the downstream work. We diagnose. We treat. We follow up. The interventions we have, from adenotonsillectomy to PAP therapy to oral appliances, make a real difference in children’s lives.
But the airway is not a passive tube that suddenly fails. It is a dynamic biological system built—or compromised—across development. The factors that determine whether it stays stable or becomes vulnerable during sleep are accumulating long before a family ever calls our office. And the window in which we can meaningfully influence that trajectory is not in the sleep clinic—it’s years earlier, in the pediatrician’s office, the orthodontist’s chair, the classroom.
Research from Guilleminault, Huang, and colleagues has documented this relationship in detail: oral-facial dysfunction in early childhood is a precursor to dysmorphic craniofacial development and, ultimately, to pediatric obstructive sleep apnea.1,2 The structural changes and the functional habits that drive them are interactive and compounding. They begin early. And they are currently managed by several different clinical specialties that rarely share a common framework.
Four systems drive this trajectory. I’ve come to think of the four systems as a developmental stack:
- each layer influencing the ones above and below it,
- each with its own critical window, and
- each currently sitting in a different silo.
Four Systems Driving the Airway Development Trajectory
Craniofacial Growth.
The dimensional architecture of the face—maxillary width, palate shape, mandibular position, the anterior-posterior dimensions of the pharynx—is largely determined during childhood, when sutural flexibility makes the skeleton genuinely responsive to functional input. This window has clinical teeth: research demonstrated meaningful improvements in sleep-disordered breathing following palatal expansion in children3—outcomes that are simply not available through the same mechanism once sutures fuse in adolescence. The intervention window is real, and it closes. By the time we’re seeing a patient in a sleep clinic, the skeletal degrees of freedom we had in childhood are largely gone.
Oral-Facial Function.
Tongue posture, swallowing patterns, and lip seal are the mechanical forces through which soft tissue shapes hard tissue during growth—what Melvin Moss articulated in his functional matrix theory4 and what subsequent craniofacial research has continued to support. A tongue resting low in the oral cavity applies deforming (rather than formative) load to the developing palate. A persistent anterior tongue thrust directs force vectors away from normal arch development.
These are not cosmetic concerns: a 2015 meta-analysis found that myofunctional therapy produced significant reductions in apnea-hypopnea index in both children and adults,5 underscoring that functional oral patterns have downstream airway consequences and intervention potential when caught early.
Breathing Mode.
Nasal breathing is the physiological default, and its developmental importance extends well beyond simple air delivery. Nasal breathing produces nitric oxide, a molecule with vasodilatory and antimicrobial properties that supports pulmonary function and oxygen exchange during sleep,6 as well as provides the mechanical stimulus for normal palatal development.
When a child shifts to chronic mouth breathing—most commonly triggered by adenotonsillar hypertrophy or allergic rhinitis—a self-reinforcing loop begins: altered breathing mechanics promote vertical facial growth that narrows the airway, which makes nasal breathing harder, which perpetuates mouth breathing. By the time this pattern is recognized, the structural feedback loop may already be well underway. What presents as a breathing habit is often a developmental trajectory.
Neuromuscular Airway Control.
The genioglossus and upper airway dilator muscles are the last line of defense against airway collapse during sleep. In infancy, this system is immature, arousal responses are inconsistent, chemoreflex sensitivity is still developing, and REM sleep, which dominates early sleep architecture, significantly reduces upper airway muscle tone. As Arens and Marcus documented in their developmental perspective on upper airway obstruction, compensatory dilator muscle activity matures through childhood.7 But a neuromuscular system asked to compensate for a structurally loaded airway from early in development may erode its reserve faster than it should. By adulthood, declining chemoresponsiveness and elevated arousal thresholds mean the last compensatory mechanism has also been spent.
What we see in the adult sleep lab is what happens when all four of these systems have been accumulating load for decades. The architecture for the 45-year-old presenting with moderate OSA was built in childhood. In many cases, the building began before anyone thought to look.
The Fragmentation Problem
Here’s what makes this clinically difficult: We have disciplines that touch each of these systems. Sleep medicine. Orthodontics. Otolaryngology. Myofunctional therapy. Pediatrics. Each is doing valid, important work.
But families navigating a child with complex airway presentations often encounter these specialists sequentially and separately. The tonsils come out. The orthodontist addresses the narrow arch a few years later. A sleep study is eventually ordered. A myofunctional therapist is found, often by a parent who looked for one (not because anyone referred them). Nobody is holding the longitudinal picture. Nobody is reading the developmental story.
The result is the underlying trajectory remains fragmented even when each individual intervention is sound. A child might receive excellent care from four different specialists and still fall through the gaps between them because there is no shared framework for connecting the timeline. No common language for flagging that the 7-year-old in front of you with habitual mouth breathing, a high-arched palate, and a history of recurrent ear infections is not just presenting with a breathing habit. She is presenting with a constellation of findings that warrant a proactive conversation between pediatrics, orthodontics, and sleep medicine—not a watchful wait.
What’s missing is what I’ve started thinking of as a front door: a shared developmental model that allows the disciplines involved in pediatric airway care to understand a child’s trajectory across time, coordinate around it, and communicate it to families clearly enough that they understand what the window of opportunity actually is—and when it’s closing.
Why I’m Writing This Now
I didn’t start my career planning to become an advocate for sleep education. I started in community college, a path that led me into training as a polysomnographic technologist, and I fell in love with sleep almost immediately.
Working overnight sleep studies gave me a front-row seat to the entire body interacting in real time. Brain waves, breathing, oxygen levels, heart rhythm, muscle tone—all changing together while someone slept. It was physiology in motion, and I was fascinated by every channel of it.
While working nights, I pursued a bachelor’s in neurodiagnostics and sleep science. Then I moved into clinical research and eventually into med-tech—working with companies developing devices and interventions for obstructive sleep apnea. Hypoglossal nerve stimulation. Surgical training. National clinical research studies. Important work, all of it, and all of it downstream.
But something kept bothering me. Almost everything in the field was built around the back half of the story. Diagnose and treat. Nobody was asking what it would mean to get to families before the diagnosis.
Then I became a parent.
Watching my son grow changed how I saw everything I thought I understood about sleep. I began noticing developmental patterns, breathing, airway development, and sleep behaviors that I hadn’t held together in the same frame before. His questions pushed me to keep learning.
Eventually, that led me to pursue further study in sleep medicine at Oxford, where access to the broader research literature helped me see the field from a wider perspective. And the more I learned, the clearer one thing became: sleep medicine has incredible diagnostics and treatments. What it doesn’t have is a front door. There is almost no early education that helps children, parents, or the clinicians who see them most often recognize how breathing and sleep shape development from the very beginning.
That realization eventually led me to create The Adventures of Watson & Sherlock, a children’s book series designed to make body literacy—especially sleep—accessible and engaging for kids and families. And it’s what led me to build Quinnspired, a pediatric sleep navigation practice built around helping families understand where they are in the developmental story and what they can actually do about it.
A Starting Point
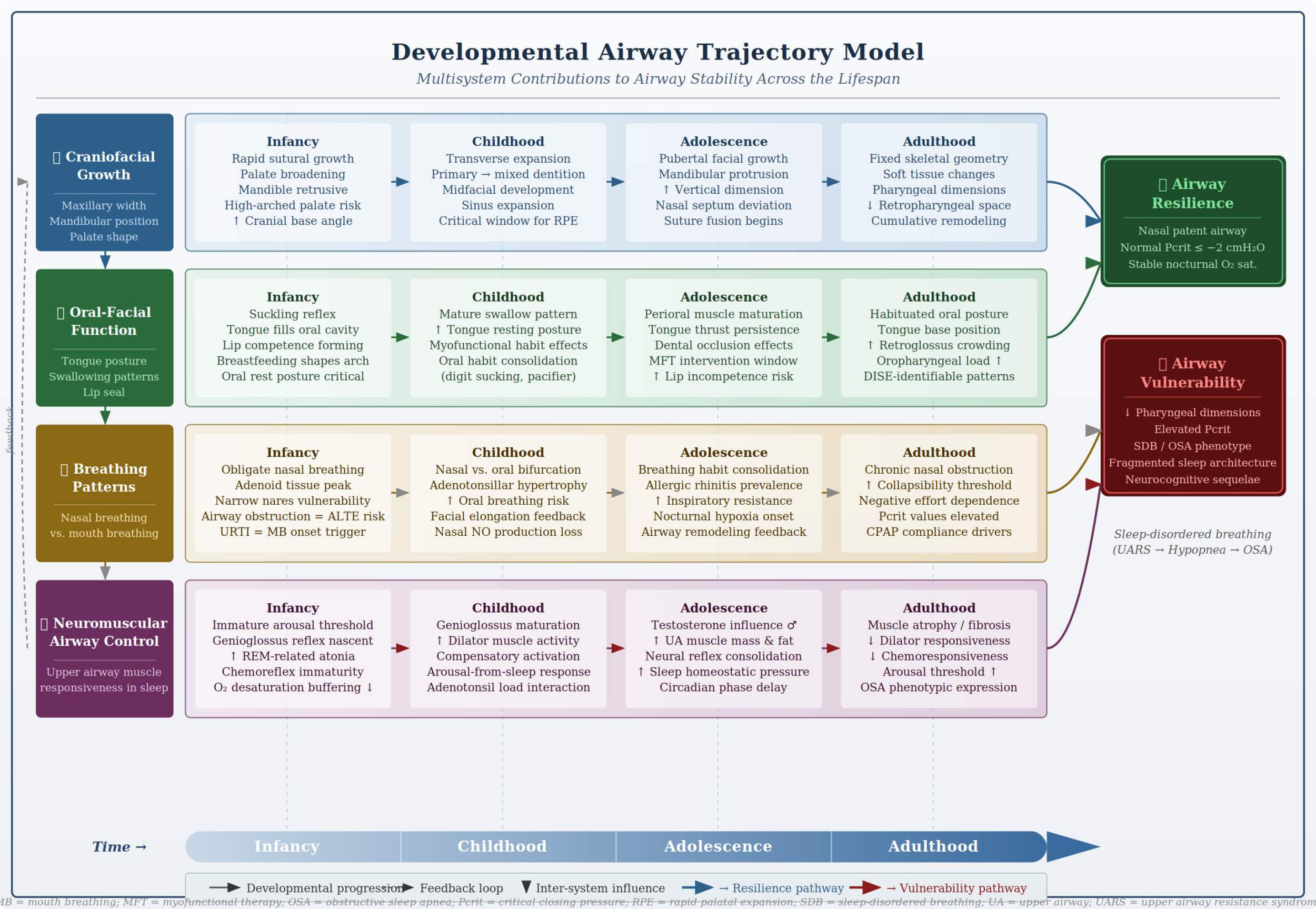
The framework I’ve outlined here, the Developmental Airway Trajectory Model, is my attempt to name what I kept seeing across years of clinical work, research, and eventually parenting: airway vulnerability is not a diagnosis. It is a developmental outcome. And developmental outcomes have trajectories. Trajectories have inflection points. And inflection points, by definition, can be influenced—if we know where to look and when.
This doesn’t require every pediatrician to become a sleep specialist or every orthodontist to conduct polysomnography. It requires a shared developmental language—one that allows the clinician who notices a child breathing through their mouth at a well-child visit to understand that observation within a developmental context, and to know which colleagues to involve and when.
My son eventually got his answer that evening. We talked about how the nose warms and filters air, how it makes a molecule called nitric oxide that helps the heart and lungs, how breathing through the nose at rest is part of how the body builds itself correctly while it sleeps. He listened, asked two follow-up questions—about normal for him—and went to bed.
Children are natural scientists. They follow the evidence without worrying about which department owns the question. The field of airway medicine could use a little more of that instinct, a willingness to follow the developmental story all the way back to where it actually begins, and to build the shared frameworks that let us act on what we find there.
The question isn’t whether the developmental trajectory matters. The evidence is accumulating across sleep medicine, orthodontics, craniofacial biology, and myofunctional therapy. What we lack is not evidence, but coordination. The question is whether we’re willing to build the infrastructure—the shared language, the referral pathways, the clinical awareness—to act on it early enough to matter.
References
1. Guilleminault C, Huang YS. From oral facial dysfunction to dysmorphism and the onset of pediatric OSA. Sleep Med Rev. 2018 Aug;40:203-14.
2. Huang YS, Guilleminault C. Pediatric obstructive sleep apnea and the critical role of oral-facial growth: evidences. Front Neurol. 2013 Jan 22;3:184.
3. Pirelli P, Saponara M, Guilleminault C. Rapid maxillary expansion in children with obstructive sleep apnea syndrome. Sleep. 2004 Jun 15;27(4):761-6.
4. Moss ML. The functional matrix hypothesis revisited. 1. The role of mechanotransduction. Am J Orthod Dentofacial Orthop. 1997 Jul;112(1):8-11.
5. Camacho M, Certal V, Abdullatif J, et al. Myofunctional therapy to treat obstructive sleep apnea: A systematic review and meta-analysis. Sleep. 2015 May 1;38(5):669-75.
6. Lundberg JO, Farkas-Szallasi T, Weitzberg E, et al. High nitric oxide production in human paranasal sinuses. Nat Med. 1995 Apr;1(4):370-3.
7. Arens R, Marcus CL. Pathophysiology of upper airway obstruction: a developmental perspective. Sleep. 2004 Aug 1;27(5):997-1019.





{kind=link}
Absolutely superb. I started reading with a “but that’s what orthopaedic dentists do” viewpoint. Then reconsidered.
It’s a fragmented care pathway and linear at best.
Dear Brooke,
First of all: BROOKE!!
Wonderful work!
This piece totally aligns with where many of us in sleep medicine are trying to go right now: internalizing the idea that airway vulnerability isn’t just a diagnosis that appears in adulthood, but a developmental story unfolding over years.
Your idea of the “missing front door” especially resonated with me. So much of healthcare fragmentation comes from the fact that families are forced to move through disconnected silos while nobody is really holding the long-term developmental picture together. Your line “Nobody is holding the longitudinal picture” says it perfectly!
I also loved the way you framed the four-system developmental stack. That kind of systems thinking feels incredibly important right now. Sleep medicine has become very good at downstream diagnosis and intervention, but the future probably depends on building collaborative models that connect craniofacial growth, breathing patterns, neurophysiology, function, and family education into one understandable narrative.
I also really liked the line about children being “natural scientists”. So true! There’s wisdom in that. Kids follow the story wherever it leads without worrying about which specialty owns the territory. Our field could use more of that “beginner’s mindset.”
What I love about your piece is that it doesn’t just point out fragmentation, but instead offers us a different way of seeing. Your piece, like Rebis, argues for a developmental framework, a shared language, and (ultimately) a more connected and humane story. That’s really what this whole dog and pony show is about, anyway!
Sending love and courage from from the Rebis corner of the world, where I can tell you first-hand, that changing a culture isn’t easy! I thought you’d like to know that this piece is deeply aligned with the broader movement toward narrative-based, collaborative, developmentally informed airway medicine, and that TEAM REBIS is all up in it!
This is an important and thoughtful piece! Thank you for writing it! 😊
Kind mojo,
Dave
David E McCarty MD FAASM
Co-creator, Empowered Sleep Apnea project (www.EmpoweredSleepApnea.com)
Chief Medical Officer, Rebis Health (www.RebisHealth.org)