
A new clinical practice guideline from the American Academy of Sleep Medicine (AASM) establishes clinical practice recommendations for the diagnosis of obstructive sleep apnea (OSA) in adults.
The guideline, which is published in the March 15 issue of the Journal of Clinical Sleep Medicine, describes the circumstances under which attended polysomnography (PSG) in an accredited sleep center or home sleep apnea testing (HSAT) should be performed for suspected OSA. Developed by an expert task force of board-certified sleep medicine physicians and approved by the AASM board of directors, the guideline was based on a systematic literature review, meta-analyses, and assessment of the evidence using the GRADE methodology. A draft of the guideline was previously made available for public comment.
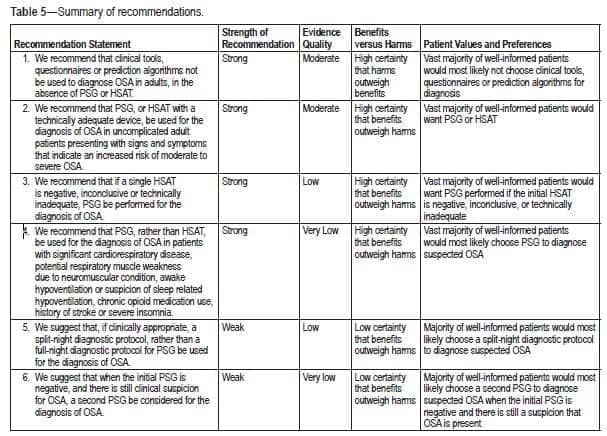
This is a summary of the recommendation statements in the Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea, including the strength of recommendation and quality of evidence. Credit: American Academy of Sleep Medicine
“This clinical practice guideline provides important recommendations for the diagnosis of obstructive sleep apnea, a chronic disease that afflicts millions of people in the US,” says AASM president Ronald D. Chervin, MD, MS in a release. “Because people who suffer from untreated sleep apnea have an increased risk of numerous health problems, including hypertension and cardiovascular disease, the accurate diagnosis of obstructive sleep apnea is essential for achieving optimal health through better sleep.”
The task force identified two “good practice statements” that underpin the provision of high quality care for the diagnosis of OSA: that diagnostic testing for obstructive sleep apnea should be performed in conjunction with a comprehensive sleep evaluation and adequate follow-up, and that PSG is the standard diagnostic test for adult patients in whom OSA is suspected based on a comprehensive sleep evaluation.
The new clinical practice guideline combines and updates recommendations from previous practice parameters and clinical guidelines published in 2005 and 2007. One of the guideline’s 6 recommendations is that both PSG and HSAT are diagnostic testing options for uncomplicated adult patients who have an increased risk of moderate to severe sleep apnea. This level of risk is indicated by the presence of excessive daytime sleepiness and at least two of the following three criteria: habitual loud snoring, witnessed apnea or gasping or choking, or diagnosed hypertension.
However, the task force found that HSAT has not been adequately validated or demonstrated to provide favorable clinical outcomes and efficient care in certain patient populations with complicating conditions. Therefore, the guideline recommends that PSG, rather than HSAT, be used for the diagnosis of OSA in patients with significant cardiorespiratory disease; potential respiratory muscle weakness due to neuromuscular condition; awake hypoventilation or suspicion of sleep-related hypoventilation; chronic opioid medication use; or a history of stroke or severe insomnia.
As the most comprehensive method of evaluating sleep, attended overnight PSG in an accredited sleep center typically measures the following parameters, which allow for the identification of sleep stages and the detection of a variety of sleep disorders: brain waves; eye, chin and leg movements; airflow, respiratory effort, and oxygen saturation; body position; and the electrical activity of the heart. HSAT uses limited-channel devices that gather less data, typically recording only airflow, respiratory effort, and oxygen saturation to identify sleep-disordered breathing. The task force states that HSAT is to be administered by an accredited sleep center under the supervision of a board-certified sleep medicine physician or a board-eligible sleep medicine provider.
Anyone who has warning signs of obstructive sleep apnea such as snoring, gasping, or choking during sleep should discuss these symptoms with a doctor.





{kind=link}
Happy to see these updates!
We see so many HSTS that are inconclusive. The level of bearocracy at these insurance companies and utilization management firms is making caring for patients very difficult. Since new years 2017, they are denying all sleep testing including HSTS for the most frivolous of reasons. The goal post is always on the move and it always seems to favor the insurance companies.