
An expert explains how to grow an underutilized sleep medicine service.
Oral appliance (OA) therapy can be as effective as CPAP for the treatment of mild to moderate obstructive sleep apnea (OSA) and can even benefit some patients with severe OSA. Although data is limited, adherence to OA therapy appears to exceed adherence to PAP, and compared to PAP, patients prefer oral appliances by a margin of 2:1.1 Yet despite these many strengths, OA therapy is underutilized.
To be clear, OA therapy should not and will not replace PAP. Even so, many factors impact the uptake of OA therapy, including scope of practice boundaries, a gross shortage of trained dental sleep providers, and a less mature evidence base relative to PAP. In my view, the single greatest barrier to more widespread adoption is a lack of perceived value from sleep medicine stakeholders.
I have coined the term “value-based sleep” to highlight the need for greater emphasis on health economic outcomes in our field and to increase focus on those that matter most to our constituents.2 Recently, I have begun to apply these same concepts to help grow dental sleep medicine and benefit patients unable to tolerate PAP. Here, I introduce the tenets of value-based dental sleep medicine.
Value Is in the Eye of the Beholder
Unlike sleep medicine professionals—who understand the many benefits of sleep and reasons to treat sleep disorders—most people only appreciate sleep as a means to an end. That is, stakeholders care about sleep only to the extent it helps them achieve their non-sleep goals. For example, patients value sleep to the extent it increases their quality of life. To provide and demonstrate value, dental sleep medicine practitioners must understand clearly the values of multiple constituents (see Table 1).
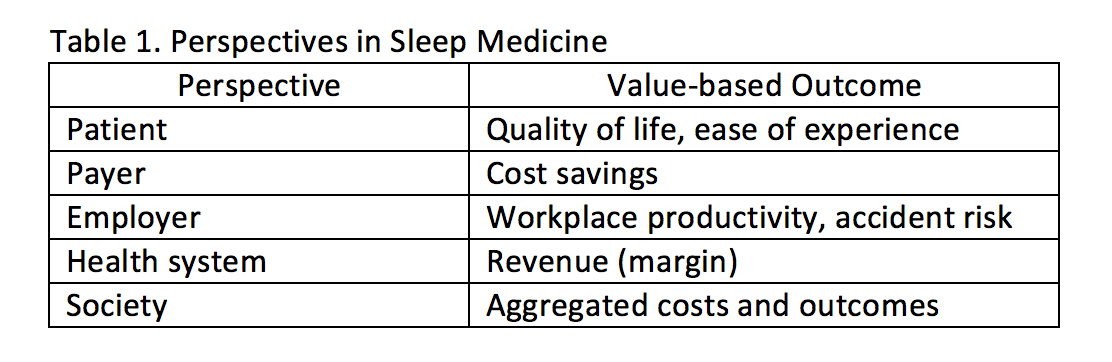
Table 1. Perspectives in Sleep Medicine. (Click on the table to make it bigger.)
3 Steps to Grow the Value of Dental Sleep Medicine
1. Adopt a patient-centered approach.
For most patients, sleep is an input, not an output. In other words, patients want to live longer, healthier, happier lives. They want more energy for recreation, enhanced cognitive function for work, and greater social connection. Yet too few dental sleep medicine practitioners know how to assess these kinds of patient-centered outcomes. Instead, the clinical and research literature has focused almost entirely on the apnea-hypopnea index (AHI). And of course, no patient cares about the AHI!
More studies are needed to identify the impact of OA therapy on quality of life, neurocognitive abilities, and cardiovascular and cerebrovascular disease risk outcomes—all of which matter greatly to OSA patients.
2. Increase focus on economic outcomes.
In a recent review of the economic impact of OSA treatments, we found only one empirical study evaluating the effect of OA on monetized economic outcomes.3 Quinnell and colleagues found that relative to no treatment, three types of OAs (self-molded, semi-custom, and fully custom) were cost-effective within a 6-week followup period.4 These promising results warrant confirmation within diverse samples of OSA patients and with longer followup periods. Even so, this finding can be viewed optimistically and suggests that OA therapy can provide a favorable economic return.
To grow the field and increase access to dental sleep medicine care, more health economic studies are needed. To increase market access, payers will need to be convinced that OA therapy can provide an important return on investment, relative to PAP and other available treatment options.
3. Develop a value-based lexicon.
For dental sleep medicine to grow, it must develop language that speaks directly to the needs and wants of patients, constituents, and partners—in terms that matter to them. This means first developing an internal mindset of “what’s in it for them?” and second, refining the external language and communication skills to highlight this value.
For most private practice dental sleep practitioners, this includes at minimum developing language for patients, referring sleep centers or other medical specialists who refer, and insurance payers. In terms of leadership of the field, expanding the scientific evidence base and clarifying the role of dental sleep medicine are paramount.

Emerson Wickwire, PhD
Final Thoughts
We live in a healthcare climate of increasing costs on the one hand and limited resources on the other. As a result, it is more important than ever for dental sleep medicine practitioners to define, demonstrate, and maximize their substantial value. This will require intense focus on the outcomes that matter to diverse stakeholders—outcomes including quality of life and reduced healthcare spend. The good news is that dental sleep medicine is poised for major growth. Thus, the time to incorporate a value-based sleep perspective into other strategic initiatives is now. Adopt a value-based dental sleep approach and survive, thrive, and grow.
[sidebar] Continue this discussion in person at the American Academy of Dental Sleep Medicine conference in San Antonio, Texas, at a session to be held on Sunday, June 9 at 8:45 am (room number to be decided; check the program closer to the date). [/sidebar]
Emerson M. Wickwire, PhD, is associate professor of psychiatry and medicine and director of the Insomnia Program at the University of Maryland School of Medicine. His current research examines health economic aspects of sleep disorders and their treatments in medical and organizational settings. His applied endeavors seek to bring the benefits of healthy sleep to all. Wickwire is associate editor of the Journal of Clinical Sleep Medicine and serves on the editorial boards of Behavioral Sleep Medicine, SLEEP, and Sleep Review.
References
1. Giles TL, Lasserson TJ, Smith BH, et al. Continuous positive airways pressure for obstructive sleep apnoea in adults. Cochrane Database Syst Rev. 2006 Jul 19;(3):CD001106.
2. Wickwire EM. Value-based sleep: a paradigm for growth and collaboration. Sleep Review. 2017 Nov 6. Available at www.sleepreviewmag.com/value-based-sleep.
3. Wickwire EM, Albrecht JS, Towe M, et al. The impact of treatments for obstructive sleep apnea on monetized health economic outcomes: a systematic review. Chest. 2019 Jan 18. In press.
4. Quinnell TG, Bennett M, Jordan J, et al. A crossover randomised controlled trial of oral mandibular advancement devices for obstructive sleep apnoea-hypopnoea (TOMADO). Thorax. 2014 Oct 1;69(10):938-45.





{kind=link}